Introduction
Hepatic steatosis represents excessive fat accumulation in the liver, whose etiology includes metabolic disease, alcohol-related, drug-induced, and cryptogenic causes1.
Metabolic dysfunction-associated steatotic liver disease (MASLD), formerly known as non-alcoholic fatty liver disease (NAFLD), is the most common cause of liver disease. MASLD is a disease that is increasing worldwide; currently, approximately 38% of adult patients with MASLD and 7-14% of children and adolescents are reported, posing a significant public health problem. By 2040, the prevalence of MASLD is projected to reach up to 55% in adults, accompanied by increasing rates of obesity and diabetes1–3.
Although MASLD does not always progress to chronic liver disease, it is the leading indication for transplantation in the United States of America, particularly in women, and with hepatocarcinoma. Cardiovascular disease (CVD) is the leading cause of mortality in patients with MASLD2.
MASLD encompasses a broad spectrum of pathologies, ranging from fat accumulation alone (isolated steatosis) to fat accumulation with associated inflammation and liver cell damage (hepatocyte ballooning), collectively referred to as metabolic dysfunction-associated steatohepatitis (MASH), formerly known as nonalcoholic steatohepatitis (NASH), and increasing degrees of fibrosis (F0-F4) up to cirrhosis. The worsening stages of the disease, from isolated steatosis to MASH with fibrosis or cirrhosis, are associated with progressively higher risks of adverse clinical outcomes4.
The progression of disease from steatosis to MASH, fibrosis, and hepatocarcinoma is heterogeneous, occurring over several years or decades, and is influenced by both nonmodifiable factors (age, sex, race/ethnicity, heredity) and modifiable factors (diet, lifestyle, medications)5.
Since MASLD is the hepatic manifestation of metabolic syndrome, it is part of a complex multiorgan disease with a bidirectional relationship that includes overlapping risk factors. Regarding the genetic factors of MASLD and CVD, several associated genetic variants have been reported, such as TM6SF2E16K and PNPLA3I148M6.
In the NHANES III (National Health and Nutrition Survey) study from 2017 to 2020, a prevalence of 35.5% was reported, and the main comorbidity was obesity at 89.1%, followed by prediabetes at 66.6%, hypertension at 50.1%, hypertriglyceridemia at 51.3%, and low high-density lipoprotein cholesterol levels at 54.7%; 65% presented three or more comorbid conditions7.
Diabetes
In diabetic patients, the prevalence of MASLD worldwide is up to 65%, compared to 38% in the global population3.
A bidirectional association has been observed between type 2 diabetes and MASLD, which increases the incidence of MASLD in diabetic patients by up to two-fold2,8.
An increase in the prevalence of MASLD in patients with diabetes has been described, from 13% in 1990-2004 to 68.8% in 2016-20212. The highest prevalences were in Western Europe (80.6%) and the Middle East (71.2%), and the lowest was in Africa (53.1%)2.
Clinical practice guidelines recommend screening by measuring the 4-factor-based fibrosis index (FIB-4), with the aim of detecting patients at high risk of developing fibrosis and liver-related complications in the presence of cardiometabolic risk factors; if the score is > 1.3, performing vibration-controlled transient elastography is suggested3,8.
In higher-risk patients, such as diabetics, it has been observed that the FIB-4 cutoff point of 1.3 allows classification of those with increased risk of hepatic complications and mortality within 5 years, considering that FIB-4 is a low-cost system with an acceptable negative predictive value but moderate sensitivity and positive predictive value. Even the 2025 American Diabetes Association guidelines mention that patients with diabetes and FIB-4 between 1 and 1.3 may have advanced fibrosis, especially if they have obesity and other cardiometabolic factors8.
In patients with biopsy-diagnosed NASH/MASH, the overall prevalence was 66.4%, of which 40.8% presented significant fibrosis and 15.5% advanced fibrosis2.
In patients with MASLD, excess insulin resistance (IR) of adipose tissue has been observed, associated with a lipid profile enriched in saturated lipids, increased macrophage activity, and greater severity of hepatic fibrosis, increasing de novo lipid synthesis, which is also favored by the metabolism of free fatty acids from the diet; the increase in de novo lipid synthesis is also observed in various metabolic diseases9.
Excessive lipid accumulation is not only due to excess free fatty acids but also to inadequate oxidation of these, but also due to mitochondrial dysfunction or decreased metabolic flexibility (ability to adapt to fluctuations in energy demand and supply to maintain body homeostasis)9.
This bidirectional effect in patients with diabetes and increased body mass index (BMI) is associated with reduced metabolic flexibility, which increases free fatty acid oxidation. In early stages of MASLD, there is a decrease in lipolysis due to increased insulin, accompanied by an increase in fatty acid oxidation and mitochondrial activity, as well as an increase in biogenesis. However, in late stages, mitochondrial respiration is reduced due to DNA and protein abnormalities9.
This vicious circle between MASLD and tissue IR is key in pathophysiology, as the metabolic consequences of IR are hyperglycemia, dyslipidemia, and increased visceral adiposity, as well as increased abdominal fat. IR decreases glucose uptake, releases free fatty acids, and suppresses the supply of non-esterified fatty acids to the liver during the postprandial period, which worsens fat infiltration in the liver, especially by toxic lipids such as ceramides. This hepatic fat accumulation causes oxidative stress, inducing endoplasmic reticulum stress, altering mitochondrial activation, with lysosomal dysfunction, inflammasome activation, cytokine release, and lipid peroxidation, causing liver damage or death10–12.
On the other hand, changes in gene expression related to MASLD and diabetes have been reported, with lower expression of the FYN, HNRNPU, and FUBP1 genes. Fyn kinase regulates intestinal epithelial permeability, and when the intestinal barrier is compromised, it allows the passage of more bacterial endotoxins, which increase hepatic inflammation and the development of steatohepatitis. The HNRNPU protein plays an important role in RNA binding, in the regulation of transcription genes, chromatin organization, and cellular response to DNA damage. This protein, together with heterogeneous nuclear ribonucleoproteins (hnRNP), modulates the expression of genes related to insulin regulation, oxidative stress, and renal function, which are highly relevant in the context of diabetes. Therefore, these proteins have a protective effect in the development of diabetes-associated complications, including hypertension and renal injury. In hepatic tissue, changes in hnRNP expression have been observed in patients with NAFLD.
Regarding the FUBP1 gene, which encodes the far upstream element binding protein 1 (FUBP1), it regulates the expression of the c-Myc oncogene, thus playing an important role in various cellular processes, including proliferation, apoptosis, and differentiation. Additionally, this protein regulates the expression of hexokinase genes (HK1 and HK2), which regulate glycolysis pathways, which are essential in glucose metabolism. Dysfunction of these pathways is directly associated with IR and alterations in glucose homeostasis. Furthermore, regulation of the c-Myc oncogene by FUBP1 protein is important in liver diseases, as it promotes the development and survival of hepatic tumor cells13.
Hypertension
It has been reported that up to 50% of patients with NAFLD or MASLD present with systemic arterial hypertension (SAH); additionally, patients with SAH and NAFLD have higher pressure levels (up to 20%), SAH is an independent factor for NAFLD, and patients with NAFLD have a higher risk of SAH incidence7,14.
In a Chinese cohort, it was observed that MASLD is associated with higher blood pressure levels, and that the effect of SAH on MASLD is lower.
In the NHANES III cohort, with a follow-up of 22.3 years, a mortality of 19.5 per 1000 person-years was observed. In patients with MASLD, the main comorbidity associated with mortality was SAH (adjusted hazard ratio [aHR]: 1.42; 95% confidence interval [95% CI]: 1.25-1.61), followed by (pre)diabetes (aHR: 1.28; 95% CI: 1.09-1.49) and hypertriglyceridemia (aHR: 1.19; 95% CI: 1.05-1.34). An important finding was that in ages 20 to 40 years, SAH was a greater risk factor (aHR: 1.96; 95% CI: 1.29-2.99), and in ages 60 to 80 years, this comorbidity was the only one associated with mortality (aHR: 1.29; 95% CI: 1.09-1.52), with SAH being the main disease as an independent predictor of mortality in all age groups7.
The mechanism by which MASLD is related to higher blood pressure levels is not completely understood; however, it has been proposed that MASLD, hepatocellular lipotoxicity, and hepatocyte damage activate the innate immune system, promoting the production of proinflammatory factors such as interleukin-6, tumor necrosis factor alpha, and CC chemokine ligand 2. These proinflammatory factors accelerate chronic inflammation, which activates the sympathetic nervous system, and this can elevate blood pressure. Additionally, the inflammatory process can also activate the renin-angiotensin system, which plays a fundamental role in the development of hypertension14.
A close relationship has been observed between type 2 diabetes, insulin levels, and IR in the possible mechanism related to increased blood pressure and MASLD, as hepatocyte damage increases IR, and this is also associated with activation of the sympathetic nervous system. Additionally, ectopic perivascular fat deposits and endothelial dysfunction promote vasoconstriction and elevated blood pressure, along with sodium reabsorption and water retention promoted by IR15.
Another possible mechanism is related to steatotic hepatocytes that release extracellular vesicles and increase endothelial inflammation and promote angiogenesis through miR-1, reduce Kruppel-like factor 4, and activate nuclear factor kappa B14.
Regarding genetic risk factors, variants associated with MASLD have been described, such as TM6SF2 E16K and PNPLA3 I148M, which cause steatosis by impeding hepatic production of triglyceride (TG)-rich lipoproteins6.
Overweight and obesity
The two main predisposing factors for prediabetes and diabetes are overweight or obesity and MASLD, with the increase in visceral adipose tissue mass being linked to these diseases8,16.
In a microphysiological study, it was observed that increased adipocyte-hepatocyte ratio affected hepatocyte function, as well as induced macrophage-mediated inflammation secondary to lipid accumulation in hepatocytes and an increase in IR, which is consistent with observations in MASLD16.
The expansion of adipose tissue related to obesity is associated with the infiltration and activation of immune cells, such as macrophages, leading to a state of chronic, low-grade inflammation17.
Both adipose tissue expansion and inflammation play important roles in the pathogenesis of type 2 diabetes through various mechanisms, including the release of cytokines that directly interfere with the insulin signaling pathway17. IR appears to be the pathophysiological link connecting obesity, type 2 diabetes, and MASLD2.
In the United States of America, up to 40% of young adults (18 to 44 years old) present with IR; this is more frequent in those with higher BMI, with hypertension or hypercholesterolemia, and of Mexican-American origin2.
The role of insulin in the development of MASLD could be related to the presence of single-nucleotide polymorphisms (SNPs) in the patatin-like phospholipase domain-containing protein 3 (PNPLA3), suggesting that individuals with MASLD and the PNPLA3 SNP are insulin-resistant and could experience more adverse hepatic outcomes due to their greater susceptibility to the effects of obesity and diabetes. Therefore, this population could need earlier and more aggressive treatment than other groups of patients with MASLD2.
Additionally, in patients with obesity, a significant increase in GDF-15 (growth differentiation factor-15), a cytokine of the transforming growth factor beta family, has been observed. This increase is controversial, as GDF-15 is an appetite inhibitor that acts in the nucleus of the solitary tract of the area postrema, yet it has been observed that GDF-15 is increased in liver samples from patients with MASLD, as well as in visceral and subcutaneous tissue from patients with obesity. Interestingly, the presence of type 2 diabetes in patients with obesity further increases GDF-15 expression in adipose tissue17.
There is an association between human adipose tissue macrophage dysfunction and the hepatic phenotype of MASLD, which proposes a new mechanism whereby aberrant differentiation and function of macrophages in adipose tissue can cause an alteration in vascular barrier integrity, potentially contributing to greater inflammatory signaling between adipose tissue and the liver in patients with MASH18.
Impact of metabolic syndrome on MASLD
In the study by Pustjens et al.7, during the follow-up period (median 22.3 years [16.9-24.2]), 1405 deaths were recorded in the MASLD population, resulting in a mortality rate of 19.5 per 1000 person-years. In multivariable analysis, hypertension, (pre)diabetes, hypertriglyceridemia, and BMI were significantly associated with all-cause mortality7. Higher mortality rates were observed for each additional cardiometabolic disorder (log-rank, p > 0.001) (Figure 1). Compared with the lowest possible cardiometabolic burden of one disorder in the MASLD population, starting from three cardiometabolic disorders, a positive association with all-cause mortality was observed. When all five cardiometabolic criteria were met, the risk of all-cause mortality was almost double that of meeting only one criterion (aHR: 1.92; 95% CI: 1.47-2.51)7.
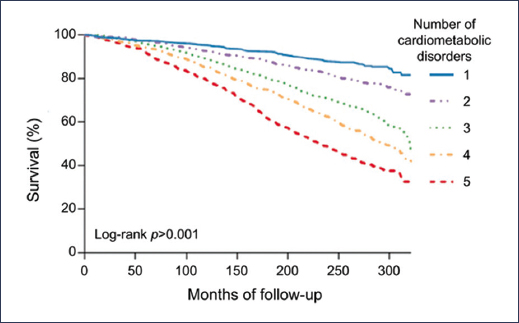
Figure 1. Survival analysis of patients with MASLD stratified by the number of cardiometabolic disorders7.
Cardiovascular disease
Fundamentally, MASLD independently increases the risk of CVD, which is the leading cause of death in this population2,19.
Shared pathways underlie the bidirectional relationship between MASLD and CVD; the ectopic fat deposition that occurs with the development of MASLD also occurs in the epicardium. In combination with the systemic inflammation present in MASLD, these factors increase endothelial dysfunction and intramyocardial inflammation, and accelerate atherogenesis, leading to coronary disease, increased risk of diastolic dysfunction and left ventricular hypertrophy, cardiac valvular calcification, arrhythmias (mainly permanent atrial fibrillation), and heart failure2,19.
Patients with three simultaneous criteria for MASLD, characterized by diabetes, obesity, and multiple metabolic abnormalities, present markedly elevated levels of low-density lipoprotein cholesterol, triglycerides, glycated hemoglobin, and atherosclerotic cardiovascular disease (ASCVD), along with advanced hepatic fibrosis indices (FIB-4 and NAFLD fibrosis score [NFS]). These findings are consistent with previous evidence positioning MASLD as a determinant factor of cardiovascular morbidity, often eclipsing hepatic sequelae in this population19.
The European Association for the Study of the Liver (EASL), the American Association for the Study of Liver Diseases (AASLD), the European Society of Cardiology (ESC), and the American Heart Association (AHA) strongly recommend CVD risk assessment in all patients with MASLD. To this end, several risk scoring systems can be used. Two 10-year CVD risk assessment scales, the Framingham Risk Score (FRS) and the Atherosclerotic Cardiovascular Disease (ASCVD) scale, are validated for use in patients with MASLD, although in relatively small studies that included only 309 and 1262 individuals, respectively6.
The SCORE2 (Systematic Coronary Risk Evaluation 2) and SCORE2-OP (older persons) models were updated by the ESC in 2021 to estimate the 10-year risk of first-onset CVD events in the European population without a history of CVD or diabetes, dividing European countries into four regional risk zones (low, moderate, high, and very high risk)6.
Patients at high or very high risk of a CVD event in the next 10 years should initiate multimodal treatments that include lifestyle changes, optimization of glycemic control, lipid-lowering drugs, antihypertensive treatment, and smoking cessation. While statin monotherapy or antihypertensive treatment should be considered in low-risk patients, if appropriate, initially it is recommended to focus on lifestyle intervention6.
Chronic kidney disease
Chronic, low-grade systemic inflammation, driven by the liver, appears to contribute not only to CVD but also to chronic kidney disease (CKD)2.
MASLD is significantly associated with a 1.45-fold increase in long-term risk of incident CKD stage ≥ 3, with MASLD being an independent predictor for CKD2.
This risk has been observed to be independent of age, sex, obesity, hypertension, type 2 diabetes, and other traditional renal risk factors. Additionally, the risk of CKD increases further with more advanced liver disease, especially with the severity of hepatic fibrosis20.
CKD is a multisystemic disease that shares numerous cardiometabolic risk factors with MASLD, making it difficult to analyze the causal relationships between both conditions, so it is likely that a complex combination of metabolic and hemodynamic changes, lipid nephrotoxicity, and genetic predisposition drives the development of CKD in people with MASLD20.
Other comorbidities
Younossi et al.2 found in their review that MASLD is associated with de novo development of diabetes, CKD, sarcopenia, and extrahepatic cancers, as well as heart failure, atrial fibrillation, and some extrahepatic cancers, with decreased quality of life, lower work productivity, fatigue, and increased use of healthcare and health resources, becoming a substantial economic burden2,3.
Conclusion
The prevalence of MASLD is increasing along with comorbidities such as obesity and type 2 diabetes, which have a bidirectional effect on the development, severity, and progression of diseases. Since MASLD is a systemic disorder with significant impacts on cardiovascular health, skeletal muscle function, and renal integrity, the approach should be multidisciplinary and personalized, prioritizing early detection and accurate risk assessment to mitigate the progression of comorbidity.
Funding
The authors declare that they received no funding for this study.
Conflicts of interest
The authors declare that they have no conflicts of interest.
Ethical considerations
Protection of humans and animals. The authors declare that no experiments were performed on humans or animals for this research.
Confidentiality, informed consent, and ethical approval. The study does not involve personal patient data or require ethical approval. SAGER guidelines do not apply.
Declaration on the use of artificial intelligence. The authors declare that they did not use artificial intelligence for the writing of this manuscript.
