Introduction
The complications of peptic ulcer disease (PUD) have changed in their frequency and presentation,1–3 due to the use of drugs such as proton pump inhibitors and, more recently, potassium blockers, as well as the eradication of Helicobacter pylori. Intestinal perforation due to peptic ulcer is generally duodenal, and its diagnosis and treatment must be as rapid as possible, since time and patient comorbidity dictate the response to treatment, primarily surgical.4 The most common gastric outlet obstruction is due to gastric adenocarcinoma, and for its treatment, when it is not surgical, endoscopic ultrasound with placement of lumen-apposing metal stents (LAMS) is more frequently used. Benign peptic strictures respond well to balloon dilation, and in some cases steroid injection is used.5,6 In gastric ulcers that do not have a good response to medical treatment, malignancy should be suspected7 (Fig. 1).
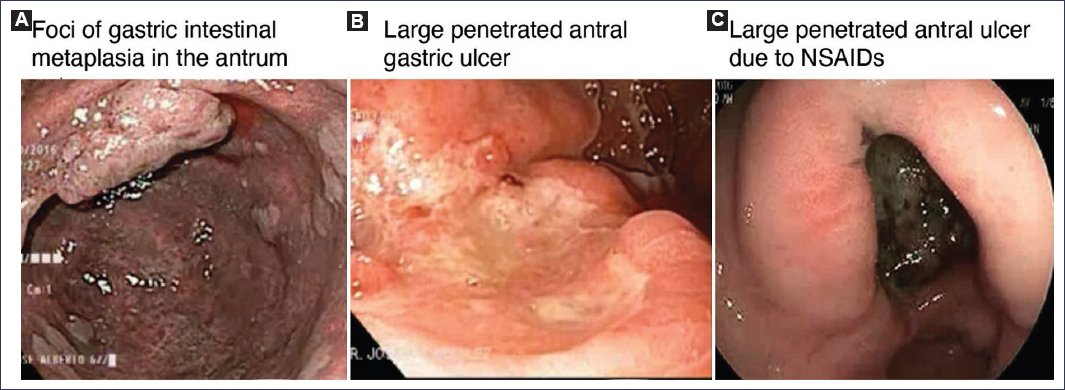
Figure 1. Endoscopic images of A: photographs of gastric metaplasia in the antrum. B: large penetrating antral gastric ulcer. C: large penetrating antral gastric ulcer (due to NSAID use). NSAID: nonsteroidal anti-inflammatory drug.
Method
The most recent published guidelines on perforation and gastric outlet obstruction, and articles on malignant transformation of gastric ulcers, were reviewed. A search was conducted in PubMed and guidelines published by the American Gastroenterological Association, the American College of Gastroenterology, the American Society for Gastrointestinal Endoscopy, and the European Society of Gastrointestinal Endoscopy (ESGE). NotebookLM was used to classify the articles.
Perforation
Hospital admission for PUD has decreased in recent times.1 One of the most serious complications is perforation, and early diagnosis and treatment are necessary to improve its prognosis2. Various risk factors for peptic ulcer are known, and some of them may increase the risk of complications, such as the presence of H. pylori. This bacterium is very common in PUD, but there are studies in which its risk factor has had contradictory results; in one it was higher in patients with perforated ulcer8 and in another it was found to be an irrelevant factor,9 with the possibility that other factors such as alcohol and tobacco abuse have greater participation, as well as chronic diseases (hepatic and renal) and drug use (cocaine).10
The increasing and continuous use of nonsteroidal anti-inflammatory drugs (NSAIDs) for chronic musculoskeletal problems is an important factor for PUD. The reported risk factors are age over 60 years, continuous use of aspirin and other NSAIDs, oral anticoagulants, antiplatelet agents or steroids, and the presence of H. pylori.
The use of cyclooxygenase-2 inhibitors, mainly in patients with low risk of cardiovascular disease, has been shown to decrease the risk of peptic ulcer. For the prevention or reduction of the risk of PUD in patients taking NSAIDs, proton pump inhibitors have been used mainly, rather than H2 blockers, due to the decrease in their efficacy attributed to tachyphylaxis in the reduction of gastric acid blockade.11 There are recommendations for the use of NSAIDs (Table 1).
Table 1. Recommendations for NSAIDs according to gastrointestinal and cardiovascular risk
| Gastrointestinal risk level | Cardiovascular risk level | Risk factors | Therapeutic recommendation | Use of PPI (proton pump inhibitors) | Suggested alternative |
|---|---|---|---|---|---|
| High | High | Advanced age, history of peptic ulcer, cardiovascular factors | If the NSAID cannot be discontinued, use non-selective NSAID with protection | Add PPI to non-selective NSAID | Avoid NSAIDs if possible |
| High | Low | Advanced age, history of peptic ulcer, high dose of NSAIDs, use of aspirin, anticoagulants, antiplatelet agents or steroids | Use of selective COX-2 inhibitor | Add PPI | Not in source |
| Low | High | High cardiovascular disease risk | Use of non-selective NSAID with caution | Add PPI to non-selective NSAID | Avoid NSAIDs if possible |
| Low | Low | Not specified | Use of NSAID (according to medical criteria) | Not mandatory | Not in source |
|
NSAID: nonsteroidal anti-inflammatory drugs; PPI: proton pump inhibitors. |
|||||
Recently, a study has been reported that compared a potassium blocker (fexuprazan, 20 mg/day) versus a proton pump inhibitor (lansoprazole, 15 mg/day), and at 24 weeks, there was no difference in the incidence of PUD (1.1% vs. 2.7%, respectively).12
Perforation due to ulcer is more frequent in the duodenum, occurring in the anterior wall in 60-67% of cases; in the stomach, the antrum and lesser curvature are the most common locations.13–15 When perforation occurs and there is gastrointestinal content in the peritoneum, this being a sterile area, chemical irritation occurs in the following 6-12 hours. The initial pain may stabilize and subsequently abdominal distension and increased pain, fever, and systemic inflammatory response data may appear.15 Some small perforations can seal spontaneously. The presence of an intestinal perforation should be kept in mind in all patients with abdominal pain, signs of peritoneal irritation, and the presence of risk factors for PUD.16 In imaging studies, plain abdominal radiograph may show Rigler’s sign (both sides of the intestinal wall are visible) and upright chest radiograph may show subdiaphragmatic free air in 80% of cases. If there are doubts, computed tomography is more sensitive, with an accuracy greater than 90%.17 The usefulness of ultrasound in various intestinal and pulmonary pathologies is increasingly being demonstrated; it can detect the presence of free air and peritoneal fluid, but its usefulness is less than that of computed tomography. Once the presence of free air has been diagnosed and perforation clinically confirmed, the patient should be staged using various clinical data and scales. The Peptic Ulcer Perforation Score (PULP) allows prediction of the risk of 30-day mortality; it evaluates age (over 65 years), comorbidity, use of corticosteroids, shock state on admission, and delay in admission (> 24 h). Other scales are also used, such as the perforated peptic ulcer analyzing project (PPAP), developed in Japan, for postoperative risk, the American Society of Anesthesiologists (ASA) scale, and others that evaluate the severity of peritonitis, such as the Mannheim Peritonitis Index (MPI), and scales such as the Sequential Organ Failure Assessment (SOFA), the Acute Physiology And Chronic Health Evaluation II (APACHE II), and the Charlson comorbidity index.18–20
The reference treatment for perforation is surgery, but there are patients in whom conservative treatment may be initially indicated. Once the patient has been staged, in selected cases conservative treatment can be carried out. This was described by Herman Taylor in 1946 and has been reported with success in 40-80% of cases.21 Candidate patients are those with less than 12 hours of evolution, hemodynamically stable, without severe comorbidity, and under 70 years of age, because it has been estimated that in those older than this age, failure when using conservative treatment is very high (67%). Being a requirement and that in a contrast study there is no leakage of contrast medium, indicating that the perforation is sealed, treatment is indicated with nasogastric tube with continuous aspiration, intravenous fluids, broad-spectrum antibiotics, acid antisecretory medications, and strict clinical and radiological monitoring, always watching for the presence of hemodynamic decompensation, increased abdominal pain or abdominal distension to, if necessary, change the treatment. It is worth mentioning that in perforation of the posterior duodenal wall, being retroperitoneal, clinical signs may be minor. In laboratory examinations, it is common for there to be leukocytosis and a slight elevation of amylase, as well as C-reactive protein. Surgery is the method of choice in these patients, but there is no specific surgical technique as the best for all cases, since this depends on the time of evolution, the general state of the patient, and their comorbidity. The most accepted is primary closure of the perforation plus omental patch, with its variants: Cellan-Jones technique (pedicled patch) or Graham patch.20
Regarding performing an open or laparoscopic approach, the latter has gained ground and is currently the first option in general, especially in hemodynamically stable patients.19 The open technique is considered if for some reason laparoscopy cannot be carried out, or when for various situations during the laparoscopic procedure it is decided to switch to open technique. When the perforation is less than 2 cm, primary closure alone with or without omental patch can be indicated; apparently, the results are similar in these cases with or without patch. When the defect is greater than 2 cm, there is a greater risk of leakage, and it may be decided to perform an antrectomy plus vagotomy; currently, this procedure has decreased its indication due to the efficacy of acid-blocking drugs and H. pylori eradication. In recent reports of endoscopic treatment for perforated ulcers, clips over the endoscope have been used.20–23
Obstruction
One of the complications in PUD, generally with a longer time of evolution, is gastric outlet obstruction, especially due to an ulcer located in the prepyloric area or in the first duodenal portion. It is characterized by a mechanical blockage at these sites, which will prevent the passage of gastric contents to the duodenum.24,25
Obstructions are divided into malignant and benign; currently, malignant ones are the most frequent (50-80% of cases).26 The main cause is gastric adenocarcinoma, and other etiologies are pancreatic cancer, duodenal or periampullary tumors, and infiltrative lesions such as lymphomas or metastatic carcinomas. The benign etiology in PUD has been decreasing in frequency due to the use of acid blockers and H. pylori eradication.
Other causes of obstruction are caustic ingestion, stenosis due to chronic pancreatitis, and less frequently pancreas divisum. Clinically, it manifests with prandial fullness, belching, vomiting, and oral intolerance. On physical examination, there is a characteristic gastric succussion or splash sign, especially in patients with benign obstruction, with gastric dilatation plus progressive weight loss. Abdominal radiograph in two positions shows the gastric bubble and the size of the stomach, but does not easily define the site of obstruction; for this, studies such as esophagogastroduodenal series with contrast medium (preferably water-soluble) and computed tomography with oral and intravenous contrast allow better definition of the characteristics of the gastric wall and the site of possible obstruction, as well as the presence of lymph nodes or suspected metastases. Once gastric outlet obstruction has been determined by clinical and radiological data, an upper endoscopy is indicated, which should be carried out once the stomach is empty of gastric contents; if it is not, a nasogastric tube should be placed and the necessary gastric lavages performed to clean the stomach as best as possible. To determine whether the lesion obstructing the lumen is benign or malignant, it is necessary to take biopsies; it is extremely important to have small-diameter endoscopy equipment and sometimes to perform the study under fluoroscopic control. Once the etiology of the obstruction and its anatomical characteristics have been established, the necessary treatment will be proposed.26 In benign peptic strictures, the use of dilator balloons is first-line, having a success rate of up to 90%, requiring the use of acid blockers and H. pylori eradication.27 The treatment of gastric outlet obstruction caused by the ingestion of caustic substances is particularly complex, due to the nature of the lesion, which usually produces deeper fibrosis and tighter and longer strictures than those of peptic origin, and success with endoscopic treatment is lower.28–30 Patients should be hospitalized to correct hydroelectrolyte imbalance, perform gastric decompression with nasogastric tube, and plan their nutrition and subsequent treatment. In general, first-line treatment is endoscopic balloon dilation, which should be done progressively and sometimes using fluoroscopy. The number of dilation procedures is higher than in peptic strictures and the risk of complications is also higher.
The patient with stricture of peptic origin, depending on its length and location, responds well to treatment with balloon dilation and antacid drugs; the number of sessions tends to be fewer than in the patient with a caustic lesion. The long-term response (2 years) reaches more than 70% of cases.31 Currently there are reports on steroid injection to improve the response in strictures in patients undergoing endoscopic mucosal dissection with extensive areas.32 LAMS or metallic stents are not indicated in benign strictures, but when this treatment does not work the indication is surgical, either laparoscopic or open, and the type of bypass to be performed will be decided according to the case.33 In malignant lesions, the use of therapeutic endoscopic ultrasound using gastrointestinal bypasses with LAMS34 is increasingly frequent; this is performed under certain criteria, such as the patient’s expected life span (less than or greater than 6 months). Gastroenterostomy by endoscopic ultrasound is a procedure that is being used increasingly, since it is less invasive than a surgical event and the new lumen-apposing stents (LAMS) allow their placement more easily. The performance of this technique should be by expert physicians. Its disadvantage is the presence of ascites, anatomical variants, tumor infiltration, and its non-standardization. Currently, in patients with expected survival of less than 6 months, for bypass with LAMS using therapeutic endoscopic ultrasound, a gastrojejunal anastomosis is performed.34 The advantages are shorter recovery time and shorter hospital stay, but a greater number of reinterventions. In patients with peptic stricture and more than 6 months of expected life, surgical gastrojejunal anastomosis seems to offer better palliation. In patients with pancreatic cancer and obstruction, if the expected survival is less than 3 months, a metallic stent, either LAMS or a fully covered stent by transduodenal endoscopy, is an option.35 There are various factors related to prognosis in patients with gastric outlet obstruction, such as the general state of the patient and age; those over 60-70 years have a higher risk with surgery.36,37 To consider the treatment to choose, it is necessary to individualize each case and consider nutritional status, ASA classification, etiology and stage, and the presence of severe comorbidity. There are minor complications, such as abdominal pain and bleeding without the need for transfusion, and also major ones, such as perforation (especially increased risk when dilating with balloon more than 15 mm), caustic etiology, long strictures more than 2 cm and complex ones, anastomosis leak, and severe hemorrhage with the need for transfusion.
In summary, the current trend in specialized centers is to use endoscopic ultrasound bypass as the first option when technically possible, reserving surgery for young patients with long life expectancy or when there are anatomical contraindications for the endoscopic approach.
Gastric ulcer and cancer
Duodenal ulcers (peptic) have virtually no risk of developing cancer. Gastric ulcer does present a positive association and risk of developing gastric cancer. A study by the StoP Project Consortium for gastric cancer demonstrated that there is a higher risk of developing cancer in patients with gastric ulcer, especially in those with non-cardia cancer.37–40 Cancer of the esophagogastric junction has been increasing and is associated with gastric body inflammation, which progresses to atrophy and intestinal metaplasia, decreasing acid production and increasing the risk of carcinogenesis. The presence of gastric atrophy and intestinal metaplasia is more frequent in patients with gastric ulcer than in those with duodenal ulcer.41,42
H. pylori is considered a type I carcinogen. The EUROGAST group study determined a six-fold increase in the risk of having adenocarcinoma, and 2.9% of patients with the bacterium will develop gastric cancer, compared to 0% of H. pylori-negative patients.43 There are different strains of H. pylori and some of them have been related to a higher risk of developing gastric cancer, such as the cagA genotype, the HomB strain, and the presence of the bab A2 gene, as well as the gastric inflammatory process caused by the presence of H. pylori infection.44–48 Regarding the differences between patients with duodenal ulcer and with gastric ulcer, the former requires the presence of acid and this comes from the antrum, and therefore should not have signs of atrophy in order to produce acid and places it at low risk of developing cancer; in contrast, gastric ulcer can develop in an environment of little or no acidity.49–51 When H. pylori migrates proximally (pangastritis), acid secretion decreases and this allows the bacterium to invade the gastric mucosa, accelerating the loss of glands and progression to atrophy and intestinal metaplasia. This loss of acidity allows the formation of N-nitroso compounds that are mutagenic, favoring carcinogenesis.52
Knowing the carcinogenic role of H. pylori, its eradication in different populations has been studied to reduce or prevent the development of gastric cancer. In a systematic review that included 58,628 healthy H. pylori-positive patients, its eradication demonstrated a reduction in gastric cancer both in the group of healthy subjects and in those with previously diagnosed gastric neoplastic lesions (treated with resection), with a reduction in relative risk of 36% in healthy subjects and 48% in patients with previous gastric neoplasms.53
To decide on eradication in various populations, factors such as the incidence of gastric cancer, socioeconomic factors, when it should be performed, the pathology present in the gastric mucosa, and epigenetic factors should be considered.
The presence of intestinal metaplasia is one of the relevant factors in the development of gastric neoplastic lesions. A multicenter study conducted in the Netherlands followed 312 patients with intestinal metaplasia for 4 years, with an average age of 62 years, and found progression of metaplasia in 35%, and dysplasia or cancer in 1.9%; the relevant factors were high salt consumption (odds ratio [OR]: 1.67; 95% confidence interval [95% CI]: 0.05-2.6; p = 0.04), eating meat more than six times a week (OR: 1.25; 95% CI: 1.07-1.4; p = 0.004), tobacco use (OR: 1.76; 95% CI: 1.04-2.6), autoimmune gastritis (OR: 2.49; 95% CI: 1.04-5.8), and having a first-degree relative with intestinal metaplasia (OR: 2.01: 95% CI 1.2-3.5) were the most relevant factors.54,55
The presence of H. pylori and salt abuse can accelerate the risk of mucosal changes to gastric atrophy, which facilitates bacterial proliferation and increases the production of carcinogenic substances; in contrast, fruits and vegetables decrease it. It has been considered that 5 grams of additional salt to that ingested daily plus the intake of cured meats increases N-nitroso compounds, and having a low vitamin intake can increase the risk of developing gastric cancer by up to 12%. Therefore, patients with gastric ulcer with changes of atrophy and metaplasia can follow the route of metaplasia-dysplasia and cancer. The use of the OLGA (Operative Link on Gastritis Assessment) and OLGIM (Operative Link on Gastric Intestinal Metaplasia assessment) classifications is important in the characterization of atrophy and intestinal metaplasia. In a meta-analysis with 12,526 patients OLGA III-IV and OLGIM III-IV, an absolute risk of 4 and 5% of gastric cancer risk and dysplasia of grade, respectively, was found.56
Some strains of H. pylori, such as CagA, increase the production of interleukin and generate an infiltration of inflammatory cells, such as leukocytes and lymphocytes, and also increase oxidative stress and this damages the DNA of the gastric mucosa with chronic inflammation.57 To consider a gastric ulcer at risk or already malignant, its location, its endoscopic and radiological characteristics, and the histopathology results should be taken into account.58 In relation to location, those located in the lesser curvature or on the posterior wall of the stomach, especially in the middle part, are at higher risk, but may not be easily diagnosed as malignant (25%). One of the most important aspects to consider for malignancy in gastric ulcers are those that, once diagnosed and adequately treated, do not respond to treatment by showing a lack of healing.59
The performance of endoscopy studies to diagnose premalignant gastric lesions has not been generally defined and the guidelines of different patients issue different recommendations. In the United States of America, screening studies in the general population to diagnose intestinal metaplasia are not recommended, and it is recommended that in patients undergoing upper endoscopies, high-definition endoscopes be used and adequately, as well as eradicating H. pylori in all patients with premalignant lesions and performing follow-up every 3 years.60,61
In Mexico, the Fifth Mexican consensus on diagnosis and treatment of H. pylori infection refers to a prevalence of infection of 70% and recommends eradication in patients with first-degree relatives with premalignant gastric lesions, with tissue-associated lymphoma, patients with atrophic gastritis and intestinal metaplasia, and those with previous or active ulcer disease.62
When a gastric ulcer is found by endoscopy, it should be evaluated preferably with high-definition equipment to determine its size, the characteristics of the mucosa around the ulcer, its edges and delimitations, as well as the mucosal and vascular pattern, to subsequently take biopsies of the edge and center of the ulcer.63
It has been considered for a long time that it is more likely that a gastric ulcer has been malignant from its inception and not that it has transformed into malignant. The malignant transformation of a gastric ulcer is considered extremely rare or infrequent, so it is agreed that benign and malignant gastric ulcers share etiological, environmental factors, and mainly the presence of atrophic gastritis and H. pylori.64,65
Discussion
The complications of PUD, such as perforation and gastric outlet obstruction, despite the use of potent proton pump inhibitors and now potassium inhibitors, are very serious events, and when they occur in elderly patients they become even more relevant, so their diagnostic approach must be immediate to establish the most appropriate treatment according to each particular case. As mentioned, the treatment for perforation is usually surgical, but there are patients in whom conservative and endoscopic treatment can be considered in selected cases. In patients with gastric outlet obstruction of malignant etiology, the initial consideration is, if possible, resection or bypass surgery, but this depends on the patient’s functional status; in cases where surgery is not possible, the use of endoscopic ultrasound bypass plus LAMS has demonstrated its benefit. Gastric ulcers should be investigated using high-definition endoscopy equipment, for their characterization and biopsy. Any gastric ulcer that does not have adequate healing should be considered suspicious of malignancy.
Conclusions
Despite their decrease in frequency, PUD complications must be kept in mind. Perforation should be suspected and diagnosed early. For the approach to gastric outlet obstruction, this is divided into benign and malignant, and in each of them, the patient’s characteristics should be considered for treatment, whether conservative management with dilations, endoscopic ultrasound bypass and LAMS, or surgery. Gastric ulcers that do not improve with medical treatment are suspicious of malignancy.
Funding
The author declares that no funding was received for this study.
Conflicts of interest
The author declares that there is no conflicts of interest.
Ethical considerations
Protection of people and animals. The author declares that no experiments were performed on humans or animals for this research.
Confidentiality, informed consent and ethical approval. The study does not involve personal data, medical histories or biological samples from humans, so it does not require ethical approval. The SAGER guidelines do not apply.
Declaration on the use of artificial intelligence. The author declares that an artificial intelligence tool (Notebook LM) was used for writing the abstracts.
