Introduction
Upper gastrointestinal bleeding secondary to stress ulcers and peptic ulcer disease (PUD) continues to be one of the most important complications in critically ill patients hospitalized in intensive care units (ICUs). In the first decades of modern critical care medicine development, this event was associated with high morbidity and mortality, prolonged hospital stays and a significant increase in resource utilization, which led to the widespread adoption of acid suppression prophylaxis strategies in the ICU.1 Although advances in hemodynamic support, mechanical ventilation and strategies to initiate early enteral nutrition have substantially modified the baseline risk of gastrointestinal bleeding, its prevention remains a priority measure in critical patient care.2
Stress ulcers originate as a result of the interaction of multiple alterations involving splanchnic perfusion and the defense mechanisms of the gastrointestinal mucosa, induced by severe physiological stress inherent to the underlying critical illness. Hypoperfusion, ischemia-reperfusion phenomenon and the cytokine cascade resulting from the systemic inflammatory response favor the appearance of acute erosions and ulcerations in the upper gastrointestinal tract.3 For its part, PUD can coexist or be exacerbated during ICU hospitalization, particularly in patients with a history of peptic ulcer, severe comorbidity or use of drugs that increase risk, especially nonsteroidal anti-inflammatory drugs, steroids or anticoagulants, which together increase the risk of clinically significant bleeding.4
The introduction of pharmacological prophylaxis with histamine H2-receptor antagonists (H2RAs) and subsequently the advent of proton pump inhibitors (PPIs) were associated with a great reduction in clinically important gastrointestinal bleeding in critically ill patients.5 While it is known that up to three-quarters of these patients can develop mucosal lesions in the absence of prophylaxis, only a minority progresses to clinically relevant bleeding, particularly those with the aforementioned risk factors. With this, current trends have been focusing on transitioning from a universal prophylaxis policy toward more selective strategies, based on individual risk stratification, rational use of antisecretory medication, continuous reassessment of risk factors and timely discontinuation of treatment when these disappear, thus avoiding overuse of acid suppression in the ICU.6
Definition
Stress ulcers are defined as acute mucosal lesions of the upper gastrointestinal tract – mainly distal esophagus, stomach and duodenum – that develop in the context of critical illness as a consequence of severe physiological stress, associated with splanchnic hypoperfusion and dysfunction of gastrointestinal mucosal defense mechanisms.1 These lesions are usually characterized by multiple superficial erosions or shallow ulcerations, with diffuse distribution, and differ from classic ulcer disease in their acute onset and direct relationship with the severity of the critical state.3
From a clinical and operational standpoint, stress ulcers can manifest in a spectrum ranging from asymptomatic endoscopic lesions to clinically important gastrointestinal bleeding. The literature distinguishes three main categories: occult bleeding, overt bleeding and clinically significant bleeding.3 Occult bleeding is identified by a gradual decrease in hemoglobin; overt bleeding includes hematemesis, melena or blood aspiration (coffee grounds, hematemesis or clots) through a nasogastric tube, and thirdly, clinically important bleeding implies hemodynamic repercussion not explained by other causes, need for transfusion, significant decrease in hemoglobin, evidence of bleeding on endoscopy or need for surgical intervention to control bleeding.7,8
On the other hand, PUD in critically ill patients refers to the presence of gastric or duodenal ulcers associated with an imbalance between aggressive factors (mainly hydrochloric acid and pepsin) and mucosal defense mechanisms, which may precede hospitalization or develop during ICU stay.5 Unlike stress ulcers, lesions in this disease are usually more localized, deep and, in many cases, related to a history of peptic ulcer, Helicobacter pylori infection or chronic use of ulcerogenic drugs.6
In critically ill patients, the distinction between stress ulcers and PUD can be difficult from a clinical standpoint, since both share similar manifestations and can also coexist. Endoscopic studies performed in ICU patients have demonstrated that a significant proportion of gastric lesions observed during diagnostic or therapeutic procedures correspond to stress-related mucosal changes, even in patients receiving standard prophylaxis.4 Likewise, a history of gastric ulcer has been identified as a factor that increases the risk of mucosal lesions and bleeding during ICU hospitalization.4,6
Finally, the concept of clinically important gastrointestinal bleeding is fundamental for therapeutic decision-making. As already mentioned, it corresponds to overt gastrointestinal bleeding and the presentation of at least one of the following clinical characteristics within the first 24 hours: decrease in systolic blood pressure, mean arterial pressure or diastolic blood pressure ≥ 20 mmHg; orthostatic hypotension or tachycardia (increase of 20 beats/minute from baseline value); decrease in hemoglobin ≥ 2 g/dl; need for transfusion of ≥ 2 units of packed red blood cells; or need for vasopressors or invasive interventions (endoscopy or surgery).3,9 Contemporary clinical guidelines consider this outcome as the main preventive objective of stress ulcer prophylaxis in critically ill patients, as it allows differentiation of clinically relevant events from endoscopic findings or minor bleeding without immediate prognostic impact within the ICU.
Epidemiology
Stress ulcers and upper gastrointestinal bleeding have experienced a significant epidemiological change in recent decades, parallel to the evolution of the modern ICU. Classic studies demonstrated that, in the absence of prophylaxis, up to 70-75% of critically ill patients develop some degree of mucosal lesion of the upper gastrointestinal tract; however, only a fraction of them progresses to clinically important bleeding.3 In current practice, the incidence of this outcome has been considerably reduced, although it continues to be clinically relevant in selected subgroups of high-risk patients.1 Table 1 presents the risk groups for gastrointestinal bleeding.
Table 1. Baseline risk of clinically important gastrointestinal bleeding according to risk factors
| Risk group | Risk factors | Gastrointestinal bleeding risk (baseline, per 1000 patients) | |
|---|---|---|---|
| Clinically important | Overt | ||
| Low risk | Acute hepatic insufficiencyCorticosteroid useImmunosuppressor useAnticoagulant use*CancerMale biological sex | 10-20 | 20-60 |
| Moderate risk | Mechanical ventilation with enteral nutritionShock state†SepsisAcute kidney injury | 21-40 | 61-90 |
| High risk | Coagulopathyೠ2 moderate risk factors | 41-80 | 91-160 |
| Very high risk | Mechanical ventilation without enteral nutritionChronic liver disease§ | 81-100 | 161-220 |
|
*Includes vitamin K antagonists, direct oral anticoagulants, therapeutic doses of heparin, thrombin inhibitors, etc. †Continuous vasopressor infusion, systolic blood pressure < 90 mmHg, mean arterial pressure < 70 mmHg or lactate ≥ 4 mmol/l.‡ Platelets < 50,000, INR > 1.5 or prothrombin time > 20 seconds.§ Portal hypertension, proven cirrhosis or history of variceal bleeding.Translated and adapted from Ye et al.1. |
|||
Recent randomized clinical trials and observational studies report that the incidence of clinically important gastrointestinal bleeding in critically ill patients ranges between 1% and 4%, depending on the definition used, the population included and the presence of major risk factors.5,8 In the SUP-ICU trial, one of the largest controlled studies in this field, the incidence of clinically important bleeding was 4.2% in the group receiving placebo and 2.5% in patients receiving PPI prophylaxis, which confirms that, even in the modern era of intensive care, gastrointestinal bleeding continues to occur frequently.2
The epidemiology of gastrointestinal bleeding in the ICU also varies according to the patient’s clinical profile. Patients with sepsis, shock, coagulopathy, chronic liver disease or severe neurological injury present higher rates of bleeding compared with critically ill patients without these factors.4,7 In patients with sepsis, for example, an increased risk of gastrointestinal bleeding has been described, particularly when multiple organ dysfunction and need for vasopressor support coexist.6 Similarly, studies in surgical and cardiovascular ICUs have documented a non-negligible incidence of mucosal lesions and bleeding, up to 4.5%, even under standard prophylaxis regimens with PPIs and H2RAs.10
The widespread implementation of acid suppression prophylaxis strategies has substantially modified the epidemiological burden of clinically important gastrointestinal bleeding.11 Previously, the incidence of overt gastrointestinal bleeding in these patients was reported at 5% to 10%, depending on the clinical risk profile. Some meta-analyses have confirmed that both PPIs and H2RAs reduce the incidence of this event compared with placebo or absence of prophylaxis. PPIs report an odds ratio (OR) of 0.61 (95% confidence interval [95% CI]: 0.42-0.89) with an absolute risk reduction of –2.3% to –3.3% in high and very high risk groups, while H2RAs overall present an OR of 0.45 (95% CI: 0.27-0.79) with a risk reduction of –3.1% to –4.6% in the same patient groups. In those patients with low bleeding risk, the absolute risk reduction is low, in addition to not having demonstrated a statistically significant reduction in mortality in any risk group, which has led to questioning the utility of universal prophylaxis.12
Another relevant epidemiological factor is the increasing practice of initiating early enteral nutrition in the ICU, within the first 24-48 hours. Various studies suggest that enteral nutrition can exert a protective effect on the gastrointestinal mucosa, contributing to the reduction of bleeding risk.11 However, available evidence indicates that this effect is not sufficient to completely eliminate risk in patients with predisposing factors, so pharmacological prophylaxis continues to be necessary in selected populations.7
Risk factors
The development of stress ulcers and clinically important gastrointestinal bleeding in critically ill patients are closely related to the presence of specific risk factors, whose identification is fundamental for adequate selection of candidate patients to receive pharmacological prophylaxis. Unlike the historical practice of universal prophylaxis, contemporary evidence supports an approach based on individual risk stratification.1
Classically recognized major risk factors include prolonged mechanical ventilation and the presence of coagulopathy. Prospective studies and clinical trials have demonstrated that patients undergoing mechanical ventilation for more than 48 hours present a significantly higher risk of clinically important gastrointestinal bleeding, particularly when other severity factors coexist.2,3 Coagulopathy, defined by thrombocytopenia generally < 50,000 and prolongation of prothrombin time or increase in INR (International Normalized Ratio), is consistently associated with an increased risk of bleeding.4
Regarding patients with mechanical ventilation, the clinical trial conducted by the PEPTIC group (in which all patients were ventilated within the first 24 hours of ICU stay) demonstrated that prophylaxis, both with PPIs and H2RAs, did not significantly impact mortality or ventilator-associated pneumonia events, although the use of PPIs presented a 27% relative risk reduction for stress ulcer bleeding.13
Among associated clinical factors, shock, sepsis and multiple organ dysfunction play a central role. Splanchnic hypoperfusion secondary to circulatory shock favors gastrointestinal mucosa ischemia-reperfusion, increasing the risk of erosions and bleeding.11 In patients with sepsis, particularly those requiring vasopressor support, a higher incidence of gastrointestinal bleeding has been documented, even under standard prophylaxis regimens, in addition to higher mortality associated with antisecretory therapy use in those requiring mechanical ventilation for more than 48 hours.6
Chronic liver disease and renal insufficiency, acute and chronic, especially requiring dialysis, have been identified as relevant risk factors, probably in relation to coagulation alterations, endothelial dysfunction and accumulation of uremic toxins.4,8 Additionally, severe neurological injury and major trauma (burn victims, polytrauma patients) are associated with an increased risk of mucosal lesions, attributable to neuroendocrine mechanisms and extreme physiological stress.10
Drug use constitutes another important predisposing factor, as the concomitant use of anticoagulants, antiplatelet agents, nonsteroidal anti-inflammatory drugs or systemic corticosteroids at high doses has been associated with an increased risk of gastrointestinal bleeding, especially when there is a history of PUD or previous episodes of digestive hemorrhage, both being independent predictive factors for bleeding and lesions documented by endoscopy during ICU stay.5
In contrast, early enteral nutrition has been consistently associated with a reduction in gastrointestinal bleeding risk, as it improves splanchnic perfusion, stimulates prostaglandin production, maintains mucosal integrity and can buffer gastric acid. However, current evidence is limited, with heterogeneous studies indicating that enteral nutrition does not completely eliminate risk in patients with major factors, so it should not be considered as a substitute for pharmacological prophylaxis.11 For its part, the SUP-ICU trial showed that, even when most patients received enteral nutrition, acid suppression with pantoprazole reduced bleeding compared with placebo.2
Clinical picture
The clinical picture of stress ulcers and PUD in critically ill patients is highly variable. Most mucosal lesions associated with physiological stress occur subclinically and do not manifest with evident symptoms, especially in sedated patients, with mechanical ventilation or with alterations of consciousness state.3 This characteristic explains why a considerable proportion of gastric lesions are identified only through endoscopic studies or by biochemical alterations documented in control laboratory studies.
From a clinical standpoint, as already mentioned at the beginning of this article, manifestations can be classified into three major categories: occult bleeding, overt bleeding and clinically important gastrointestinal bleeding.
Occult bleeding is the most frequent form, up to 15% of patients, and is usually detected by a gradual decrease in hemoglobin, even with positive guaiac tests, without evident clinical evidence of hemorrhage. This type of bleeding, although common, is rarely associated with significant hemodynamic repercussion.2,3
Overt bleeding includes the presence of hematemesis, melena or blood aspiration through a nasogastric tube. It has been reported in 1.5% to 8.5% of critically ill patients.3 These manifestations can go unnoticed or be identified late, especially when the patient is sedated, with altered level of alertness or under invasive ventilatory support.4 The appearance of overt bleeding usually motivates intensification of acid suppression, achieving better results than in clinically important hemorrhage.1
Clinically important gastrointestinal bleeding represents the outcome of greatest clinical relevance. It is defined by the presence of overt bleeding accompanied by at least one of the following characteristics: hemodynamic instability (decrease in systolic, diastolic or mean arterial blood pressure, tachycardia or orthostatic hypotension), need for transfusion of two or more packed red blood cell units, significant hemoglobin drop (≥ 2 g/dl) or requirement for endoscopic or surgical therapeutic intervention.1,3 Although it is the least frequent (1% to 3%), this type of bleeding is one of the main primary objectives, as this complication entails longer hospital stays and higher mortality in ICU patients.
Various studies conducted in critically ill patients have demonstrated that endoscopic gastrointestinal mucosal injury occurs early in critically ill patients, even within the first 72 hours of ICU admission, even before presenting overt bleeding. The main findings reported in these endoscopies included gastric erosions, hemorrhagic gastritis, superficial ulcers and in lesser proportion, gastric or duodenal ulcers.5 In patients with a history of PUD, the clinical picture may be more severe with signs of hemodynamic instability, as in endoscopy the lesions may be multiple and deeper, and stigmata of recent hemorrhage may be found.
It is important to emphasize that gastrointestinal bleeding in critically ill patients rarely presents in isolation. It is frequently accompanied by other signs of clinical deterioration and multisystemic involvement: hypotension, tachycardia, signs of tissue hypoperfusion, increase in vasopressor requirements and often worsening of organ failures. Therefore, its detection through close clinical surveillance and timely management are important.
Management
The management of stress ulcers and PUD in critically ill patients is based on the prevention of clinically important gastrointestinal bleeding through adequate risk stratification and rational use of acid suppression. The evidence supporting these strategies comes from large-scale randomized clinical trials and contemporary meta-analyses, which have allowed redefining the role of prophylaxis in the ICU.
Primary prophylaxis
Primary prophylaxis is indicated in critically ill patients with established risk factors for gastrointestinal bleeding. PPIs and H2RAs are the most studied therapies and recommended by different intensive care societies, based on the results of clinical trials.1
The SUP-ICU trial, published in 2018, evaluated the effect of intravenous pantoprazole versus placebo in critically ill patients at high risk of gastrointestinal bleeding.2 This study included more than 3,200 patients from 33 ICUs and demonstrated that the use of pantoprazole was not associated with a statistically significant reduction in mortality at 90 days compared with placebo administration (31.1% vs. 30.4%). However, a 42% relative reduction in the incidence of clinically important gastrointestinal bleeding was observed, without increasing episodes of pneumonia or Clostridioides difficile infection. This landmark study was key to demonstrate that acid suppression in selected patients decreases hemorrhagic events, although it does not totally affect mortality.
Subsequently, the PEPTIC study, a multicenter clinical trial published in 2020, compared a prophylaxis strategy with PPIs versus H2RAs administration in more than 26,000 ICU patients requiring invasive mechanical ventilation within the first 24 hours of admission.13 The study found no significant differences in hospital mortality between both groups (PPI 18.3% vs. H2RA 17.5%; p = 0.054), but a trend toward a lower bleeding rate was observed in the PPI group (PPI 1.3% vs. H2RA 1.8%; p = 0.009), although the relative reduction was 27% and the number needed to treat was 196. There were no differences in time to extubation or in C. difficile infection. With this evidence, the thesis was reinforced that both pharmacological groups are valid for prophylaxis and their choice should be individualized according to the patient’s clinical profile.
Finally, the REVISE study, an international multicenter clinical trial with more than 4,800 ICU patients with mechanical ventilation, mainly due to cardiovascular and neurological diagnoses, demonstrated that the use of 40 mg of pantoprazole daily was superior to placebo in reducing clinically significant gastrointestinal bleeding events (pantoprazole 1% vs. placebo 3.5%; p < 0.001). A 70% relative reduction for bleeding was demonstrated, but there were no differences in days of mechanical ventilation, ICU length of stay or mortality between both groups. Likewise, a higher rate of infectious adverse events in the intervention patients was not demonstrated.14
In relation to this evidence, other contemporary meta-analyses have confirmed that pharmacological acid suppression reduces the risk of clinically important gastrointestinal bleeding compared with placebo or absence of prophylaxis, without an increase in nosocomial infections; however, an important effect on overall mortality has not been demonstrated.5,15
Another strategy that has been proposed for the reduction of overt bleeding risk is early initiation of enteral nutrition. While there are few clinical trials that include this maneuver as primary treatment, current evidence indicates that it does not replace pharmacological prophylaxis in these patients.11
Secondary prophylaxis
Secondary prophylaxis is applied in patients who have presented an episode of gastrointestinal bleeding during their ICU stay or who show lesions and stigmata with high bleeding risk on endoscopy. In this clinical context, acid suppression should be intensified, generally with PPIs, until the patient presents hemodynamic stability.8
Although available clinical trials do not specifically focus on treatment strategies after a hemorrhagic event, data derived from studies such as SUP-ICU suggest that acid suppression reduces the recurrence of clinically important bleeding in patients who have already presented mucosal lesions.9 In patients with previous PUD, this approach is particularly relevant due to the higher risk of recurrence during the critical phase.10
Tertiary prophylaxis
Tertiary prophylaxis is oriented toward preventing recurrences and, equally important, avoiding overuse of acid suppression. Observational studies and analyses derived from large clinical trials have documented that a considerable proportion of patients continue to receive PPIs or H2RAs after resolution of critical illness, without a clear indication.11
Contemporary clinical guidelines recommend discontinuing stress ulcer prophylaxis when risk factors have disappeared and emphasize the need to reassess its indication before ICU discharge.12 This strategy seeks to balance the preventive benefit of gastrointestinal bleeding with minimization of potential risks and inappropriate long-term prescription. Figure 1 shows a flow diagram summarizing the decision to initiate pharmacological prophylaxis for stress ulcers (Table 2).
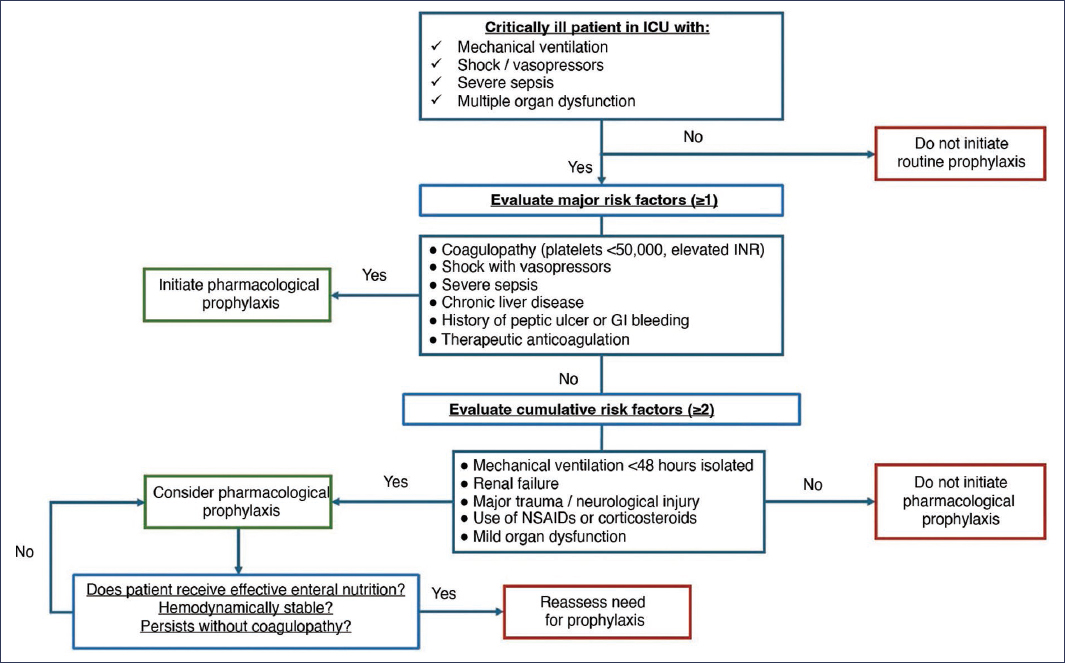
Figure 1. Algorithm to decide initiation of prophylaxis for stress ulcers.
Table 2. Therapeutic options for stress ulcer prophylaxis
| Route of administration | Proton pump inhibitors | H2-receptor antagonists | Cytoprotective agents |
|---|---|---|---|
| Parenteral | Omeprazole 40 mg/day Pantoprazole 40 mg/day Esomeprazole 40 mg/day |
Famotidine 20 mg/12 h | – |
| Enteral | Pantoprazole 40 mg/day Omeprazole 40 mg/day Lansoprazole 30 mg/day Esomeprazole 40 mg/day |
Famotidine 20 mg/12 h Cimetidine 300 mg/6 h Ranitidine 150 mg/12 h |
Sucralfate 1 g/6 h |
|
Only tablet formulations can be crushed and administered through feeding tubes; this is not applicable to capsules or enteric-coated tablets. Translated and adapted from Saeed et al.3. |
|||
Prognosis
The prognosis of critically ill patients who develop stress ulcers or PUD largely depends on the appearance of clinically important gastrointestinal bleeding, as well as the severity of the underlying disease and the presence of multiple organ dysfunction. Although the overall incidence of gastrointestinal bleeding has decreased in the modern era of intensive care, its occurrence continues to be associated with relevant clinical consequences.1
Various studies have demonstrated that clinically important gastrointestinal bleeding is related to an increase in the need for packed red blood cell transfusion, greater requirement for hemodynamic support and prolongation of ICU stay.2,3 These factors, although not always translated into a direct increase in mortality, reflect greater clinical complexity and notable hospital resource consumption.
Regarding mortality, large randomized clinical trials have shown consistent results. The SUP-ICU study found no significant differences in mortality at 90 days between patients treated with pantoprazole and those who received placebo, despite observing a reduction in the incidence of clinically important gastrointestinal bleeding in the prophylaxis group.4 Similarly, the PEPTIC study did not identify significant differences in hospital mortality when comparing prophylaxis strategies with PPIs versus H2RAs.5
Contemporary meta-analyses confirm these findings, indicating that, although prophylaxis with acid suppression reduces the risk of clinically important gastrointestinal bleeding, it is not associated with a consistent reduction in overall mortality in critically ill patients.6,7 This observation suggests that ICU mortality is determined to a greater extent by the underlying critical illness and the magnitude of organ dysfunction, rather than by the isolated occurrence of gastrointestinal bleeding.
However, the prognostic impact of gastrointestinal bleeding should not be underestimated. Observational studies have documented that patients who develop clinically important bleeding present a more complicated evolution, with higher frequency of adverse events and delay in functional recovery.8 In specific subpopulations, such as patients with sepsis, shock or chronic liver disease, gastrointestinal bleeding can act as an additional decompensating factor, contributing to clinical deterioration.9
In relation to complications associated with the use of acid suppression, large-scale clinical trials have not demonstrated a consistent increase in serious infectious events or in mortality attributable to treatment, which supports the overall safety of prophylaxis when used appropriately.10 However, prolonged and unnecessary use of these drugs beyond the critical phase may expose patients to potential risks without clear benefits.
Overall, the prognosis of stress ulcers and PUD in critically ill patients is closely linked to the prevention of clinically important gastrointestinal bleeding and to the evolution of the underlying critical illness. Adequate prophylaxis contributes to reducing hemorrhagic events and associated complications, although without consistently modifying overall mortality, which reinforces the need for a rational preventive approach based on risk stratification.
Conclusions
Stress ulcers and PUD continue to be relevant in critically ill patients, particularly due to their association with clinically important gastrointestinal bleeding. Although the overall incidence of this event has substantially decreased in the modern era of intensive care, its appearance continues to have significant clinical implications, especially in patient subgroups with well-defined risk factors.
Current evidence demonstrates that prophylaxis with acid suppression reduces the incidence of clinically important gastrointestinal bleeding in selected critically ill patients; however, a consistent benefit in overall mortality is not observed, which underscores that the main objective of prophylaxis should focus on the prevention of hemorrhagic events and their complications, rather than on direct modification of vital prognosis.
In contrast, the evidence does not support the indiscriminate use of prophylaxis in critically ill patients at low risk, especially in those receiving adequate enteral nutrition and presenting hemodynamic stability.
PPIs and H2RAs have demonstrated to be effective options for stress ulcer prophylaxis, without conclusive evidence of an increase in serious adverse events or mortality.
Overall, the management of stress ulcers and PUD in critically ill patients should be based on an individualized strategy, supported by risk stratification, integration of clinical evidence and dynamic reassessment of the patient during their ICU stay. This approach allows maximizing the benefits of prophylaxis, minimizing potential risks and optimizing the use of resources in the care of critically ill patients.
Funding
The authors declare that they have not received funding for this study.
Conflicts of interest
The authors declare no conflicts of interest.
Ethical considerations
Protection of human and animal subjects. The authors declare that no experiments were performed on human beings or animals for this research.
Confidentiality, informed consent and ethical approval. The study does not involve personal data, medical records or human biological samples, so it does not require ethical approval. SAGER guidelines do not apply.
Declaration on the use of artificial intelligence. The authors declare that no type of generative artificial intelligence was used for the writing or creation of content of this manuscript.
