Introduction to the role of diet in irritable bowel syndrome
Since 70%-89% of patients with irritable bowel syndrome (IBS) report exacerbation of symptoms with certain specific foods, it is common for them to self-eliminate these foods from their diet, negatively impacting their nutritional status1. Therefore, diet is a fundamental pillar in the management of IBS. As first-line therapy, the implementation of dietary and lifestyle changes according to the guidelines of the National Institute for Health and Care Excellence (NICE) is recommended (shown in Table 1). As second-line therapy, a restrictive diet such as the low fermentable oligosaccharides, disaccharides, monosaccharides, and polyols (FODMAP) diet is suggested2. This dietary intervention represents the approach with the greatest scientific evidence for IBS treatment, but due to its complexity, different nutritional strategies continue to be studied with the goal of finding one that facilitates patient adherence. Less restrictive dietary approaches, without disruption of the microbiota or micronutrient status, are the alternatives currently being proposed.
Table 1. General recommendations from the National Institute for Health and Care Excellence (NICE) guidelines
| Eat meals regularly |
| Avoid prolonged fasting (> 4 hours) |
| Do not skip meals |
| Drink 8 glasses of water per day |
| Limit caffeine intake to a maximum of 3 cups per day |
| Limit fresh fruit consumption to 3 portions per day |
| Reduce intake of processed foods |
| Avoid artificial sweeteners (ending in -ol) |
Low-FODMAP diet: the best strategy?
Principles of the diet and its clinical efficacy
The low-FODMAP diet is a dietary intervention that reduces the intake of fermentable oligosaccharides, disaccharides, monosaccharides, and polyols, aiming to decrease osmotic pressure and bacterial fermentation in the intestine. It is currently the dietary intervention with the strongest scientific support for IBS management.
Multiple meta-analyses have shown significant improvement in global symptoms with a low-FODMAP diet vs traditional diets. One meta-analysis reported a risk ratio of 1.21 (95% confidence interval, 0.98-1.51) for global symptom improvement with the low-FODMAP diet, particularly in abdominal pain and bloating, although with significant heterogeneity among studies (I² = 63%)3.
Elimination and reintroduction process
This dietary regimen consists of 3 phases:4
- Elimination phase: All FODMAPs are restricted for approximately 4-8 weeks. The diet is considered low when intake is < 0.5 g per serving or < 3 g/day5. Proportions for this restriction are shown in Table 26.
- Reintroduction phase: Each FODMAP group is progressively reintroduced in a non-cumulative fashion to avoid additive effects and to identify individual tolerance to each group. When a group or specific food that triggers classic symptoms is identified, it should be removed again, and its definitive elimination considered5.
- Personalization phase: Foods containing FODMAPs may be consumed according to individual tolerance, thereby controlling symptoms5. (Table 3)
Table 2. Proportions of a low-FODMAP diet
| < 0.3 g per serving of oligosaccharides (grain-based products, legumes, nuts, and seed oils) or less than 0.2 g per serving of oligosaccharides (legumes, nuts, seeds, fruits and vegetables, grain-based products) |
| < 0.4 g per serving of total polyols |
| < 0.4 g per serving of excess fructose |
| < 1 g per serving of lactose |
Table 3. Food Tables according to FODMAP content6
| Low | Moderate | High | |
|---|---|---|---|
| Vegetables | Swiss chard Alfalfa Arugula Broccoli Pumpkin Chayote Chili Green beans Spinach Soybean sprouts Corn smut (huitlacoche) Jicama Cucumber Peppers Carrot |
Eggplant White cabbage Red cabbage Tomato Kale Lettuce |
Artichoke Celery Garlic Beet Onion Mushrooms Peas Brussels sprouts Cauliflower Asparagus Fennel bulb Radishes Oyster mushrooms Shallot |
| Fruits | Blueberries Strawberries Kiwi Lemon Mandarin Melon Orange Papaya Pineapple Dragon fruit (pitaya) Tamarind Grapefruit Grapes |
Date (2 pieces) Guava Banana |
Cherries (1 cup) Plum Peach Raspberry (1 cup) Pomegranate Fig Mango Apple Nectarine Pear Watermelon (1 cup) Blackberry (⅔ cup) Dried fruit |
| Dairy | Lactose-free milk Butter Hard cheeses (manchego parmesan) Lactose-free yogurt Greek yogurt |
Cottage cheese Fresh cheese |
Kefir (200 ml) Condensed milk Whole milk Evaporated milk Cream cheese Regular yogurt |
| Cereals | Amaranth Rice Oats Corn flakes Sweet potato Corn Popcorn Potato Quinoa Rice cakes Corn tortillas |
Barley Rye Couscous Wheat and derivatives (bread flour pasta semolina) |
|
| Fats | Vegetable oils (canola sunflower olive) Peanut Mayonnaise Nuts Pumpkin Sunflower and Chia seeds |
Avocado Almond Dried coconut Cashew Pistachio |
|
| Legumes | Hummus Edamame | White beans Common beans Fava beans Lentils Textured soy Soft tofu |
|
| Beverages | Coffee Juices/smoothies (allowed fruits and vegetables) White tea Matcha tea Mint tea Green tea |
Commercial coconut water Coffee with whole milk Syrups Fruit juices (apple orange) Kombucha Regular or diet sodas Chai tea Fennel tea |
|
| Sugars | White sugar Brown sugar Dark chocolate Glucose Maple syrup Natural stevia |
Honey (1 teaspoon) Jams | Milk chocolate Fructose Agave syrup High-fructose corn syrup Mannitol Sorbitol |
| Animal-based foods | Low content: all (lamb, pork, beef, eggs, seafood, fish, turkey, chicken, veal) | ||
| Condiments | Low content: cilantro, parsley, basil, dill, oregano, cinnamon, clove, cumin, turmeric, curry, mint, mustard, paprika, rosemary, sriracha (1 teaspoon), soy sauce (2 tablespoons), vanilla, vinegars | ||
|
Source: Monash University App© . |
|||
Long-term benefits and limitations
In a meta-analysis including 6 randomized clinical trials with a total of 182 patients on a low-FODMAP diet and 172 patients on a standard habitual diet, bloating and other GI symptoms were evaluated at baseline and at 3 and 6 weeks7. The meta-analysis found a significant reduction in bloating, measured by the IBS Symptom Severity Score (IBS-SSS), in patients on the low-FODMAP diet7.
Another meta-analysis of 12 randomized clinical trials assessed the effect of a low-FODMAP diet on GI symptoms, including both objective and subjective bloating, comparing 3-6 weeks of a low-FODMAP diet with any other dietary intervention8. The meta-analysis concluded that the low-FODMAP diet produced the greatest improvement in bloating vs other dietary interventions8.
Certain limitations and disadvantages have been observed, including its impact on intestinal microbiota, low patient adherence, the need for trained health professionals (dietitians or physicians) for its implementation, and the lack of standardization of FODMAP content in foods in Mexico9.
Patients on a low-FODMAP diet long-term are at risk of nutrient deficiencies (calcium, iron, zinc, vitamin D, folates, and thiamine). For this and other reasons, management should always be guided by a dietitian or specialist10.
The patient should always be approached in an individualized manner, avoiding standardized diets, while considering the availability of time and access to foods to foster patient interest and adherence; otherwise, there is a risk of little or no compliance.
Impact on the intestinal microbiota
By restricting a wide variety of foods, the intestinal microbiota is negatively altered, with reductions in Bifidobacteriumand Faecalibacterium prausnitzii and increases in Clostridium species. Reduced intake of fiber and antioxidants (flavonoids, carotenoids)2 may lower concentrations of certain short-chain fatty acids such as propionic and valeric acids, which are important for intestinal health11,12.
Food intolerances in irritable bowel syndrome
Lactose, fructose, sorbitol, and gluten: common culprits?
In addition to FODMAPs, several foods and dietary patterns are associated with intolerances that may worsen IBS symptoms. Fructose malabsorption—present in fruits, honey, syrups, and processed foods—can cause symptoms due to colonic fermentation when luminal fructose exceeds the absorptive capacity of enterocytes. Humans have a lower absorption capacity for fructose compared with glucose; however, in combination with glucose, absorption is increased due to Na+-glucose cotransport.
Fructose malabsorption occurs when free fructose exceeds absorptive capacity, particularly when fructose exceeds glucose. There is wide interindividual variability: between 10% and 55% of healthy individuals do not completely absorb 25 g of fructose, whereas smaller doses are usually well tolerated. Unabsorbed fructose reaches the colon, where it undergoes fermentation13.
Diagnostic methods for food intolerances
The clinical utility of breath tests is debated, as patients may improve on a restrictive diet without positive test results, and vice versa. This highlights diagnostic complexity and the need to evaluate clinical symptoms alongside test results, also considering dietary context and interactions with other carbohydrates14.
On the other hand, there is insufficient evidence to recommend allergy panels measuring food-specific IgG, despite frequent patient requests. According to current clinical practice guidelines, serum food-specific IgG4 only indicates repeated exposure to food components and does not represent allergy, intolerance, or sensitivity; thus, its use should not be recommended14,15.
Fiber and irritable bowel syndrome: ally or enemy?
Dietary fibers are plant-based carbohydrates that cannot be digested by the human body and have different impacts depending on their functional characteristics. Fibers can be categorized according to their solubility into two types: soluble and insoluble. They can also be classified by their degree of fermentability, and rapidly fermentable fibers (such as fructans and galactooligosaccharides) may generate symptoms in individuals with visceral hypersensitivity, so their restriction may reduce colonic fermentation and relieve symptoms in IBS and functional dyspepsia. However, limiting colonic fermentation may slightly affect the composition of the microbiota, which can be restored with the gradual reintroduction of fermentation.
Scientific evidence has shown that dietary fiber plays an important role in intestinal inflammation, due to its fermentation into short-chain fatty acids within colonocytes. These short-chain fatty acids contribute to greater diversity in the intestinal microbiota and protect against intestinal dysbiosis16. Based on this, it is postulated that low-fiber diets promote intestinal inflammation, while high-fiber diets protect against inflammatory processes
Fibers such as psyllium, wheat bran, nopal fiber, and sugarcane bagasse may benefit IBS patients with constipation-predominant IBS. Psyllium and nopal are poorly fermentable and better tolerated than wheat bran. Nopal fiber improved overall symptoms but did not affect laxation17. Fermentable fibers, such as fructans, galactooligosaccharides, and polydextrose, have little effect on constipation17.
Supplementation with fermentable fibers (3–24 g/day) in patients with DGBI, such as IBS, may promote the growth of beneficial bacteria like bifidobacteria. However, this modulation of the intestinal microbiota does not always translate into an improvement in GI symptoms in patients with DGBI.
Gluten-free diet in IBS: valid strategy or passing trend?
In a study of self-reported non-celiac gluten sensitivity, fructans—not gluten—triggered GI symptoms18. No significant difference was found between gluten and placebo groups, whereas fructans produced greater symptoms. This suggests fructans may be the true triggers in these patients, casting doubt on the need for a gluten-free diet in those self-diagnosed with gluten sensitivity18.
The available scientific evidence regarding a gluten-free diet for patients with IBS, especially those with diarrhea predominance, is limited and often of low quality to recommend its use. Although some patients may experience symptom improvement with a gluten-free diet, this is insufficient to recommend it in a generalized manner. Further research is needed to better understand the mechanisms and efficacy of such dietary interventions19,20.
Table 4 illustrates the existing evidence on these and other dietary interventions for treating IBS symptoms is summarized.
Table 4. Evidence on other diets used to treat irritable bowel syndrome
| Type of diet | Description | Evidence |
|---|---|---|
| Lactose-free | Avoid any product containing lactose for 2 weeks; if symptoms improve, continue lactose-free diet. If symptoms persist, lactose-containing foods may be reintroduced. | Useful for patients with lactose intolerance; not effective for IBS patients without lactose intolerance. |
| Low/free fructose | Avoid foods high in fructose and fructans. | Observational studies and randomized clinical trials. Beneficial effects on symptoms, but dependent on adherence. |
| Data limited to IBS patients with breath tests or fructose malabsorption. | ||
| Gluten-free | Eliminate wheat, barley, and rye in any form. | Insufficient evidence to recommend in IBS patients. |
| IgG-based | Eliminates foods with elevated IgG antibody levels. | Compared with healthy controls, IBS patients appear to have higher IgG antibody levels; however, symptom severity does not correlate with antibody titers. |
| On an IgG elimination diet, IBS patients experienced a small symptom reduction, varying with adherence (10–26%) vs a sham diet. | ||
| Very low-carbohydrate or ketogenic | < 20 g/day of carbohydrates, 5% of daily calories (vs mean of 55%). | Only one study with 13 IBS patients with diarrhea predominance; 77% noted symptom improvement, specifically in frequency and consistency of bowel movements, quality of life, and pain scores. |
| Fiber supplementation | Psyllium, gradual increase (2–3 g/day) of soluble fiber intake from diet or supplements. | Several randomized clinical trials and meta-analyses. |
| Soluble fiber is slightly more effective than placebo for IBS symptom management; insoluble fiber is ineffective. | ||
| Low-fat | < 27 g/day, based on a 2000 kcal diet. | Some observational studies and uncontrolled trials, but no randomized clinical trials. |
| A high-fat diet can induce symptoms in IBS subjects. Reducing fat intake may benefit patients who associate meals with pain. | ||
| Low-fiber | <10-15 g/day. | No available evidence; common practice recommends reducing fiber in patients with diarrhea to increase transit time. |
| Low-histamine | Reduce intake of histamine-liberating foods: alcohol, eggs, fish, meat, aged cheeses, nuts, certain fruits, chocolate. | No evidence supporting its utility in IBS. |
|
IgG: immunoglobulin G; IBS: irritable bowel syndrome. Based on Werlang et al.¹ |
||
Role of the microbiota in dietary response
Gut dysbiosis and symptom influence
Intestinal dysbiosis is associated with IBS through various mechanisms. Several studies have shown that populations with IBS present a characteristic pattern in the intestinal microbiota. Specifically, in constipation-predominant IBS there is an increase in Firmicutes (Clostridium spp.), Alistipes, and Butyricimonas, whereas the diarrhea-predominant IBS subtype shows an increase in Enterobacteriaceae, Acinetobacter, Butyricimonas, and Odoribacter, along with a decrease in fecal microbiota diversity.
It has been demonstrated that the fecal microbiota of subjects with IBS differs significantly from that of healthy subjects (p < 0.0253) and may influence colonic transit, contributing to alterations in bowel patterns21.
Use of probiotics and prebiotics in the dietary management of IBS
The use of probiotics and prebiotics in IBS has variable support depending on the subtype of the disease and the specific strains used. Scientific evidence suggests that probiotics may be effective in improving IBS symptoms, while prebiotics have not yet shown clear benefits.
Specifically, the strain Bifidobacterium infantis 35624 has been shown to normalize the abnormal ratio of interleukins 10 and 12, and to relieve IBS symptoms, except for stool frequency and consistency, with a dose-dependent effect. Other strains with evidence of improvement in abdominal pain, bowel frequency, and quality of life in patients with diarrhea-predominant IBS are Lactiplantibacillus plantarum and Bacillus coagulans. In constipation-predominant IBS, administration of Lactobacillus helveticus for 1 week improved abdominal symptoms associated with constipation and reduced intestinal transit time22.
Specific strains associated with abdominal pain reduction in IBS include Bacillus coagulans MTCC5260, Saccharomyces boulardii CNCM I-745, Saccharomyces cerevisiae CNCM I-3856, and Lactiplantibacillus plantarum 299v. However, for abdominal bloating, the level of evidence on the benefit of combining strains was very low22.
Due to study heterogeneity and the low quality of evidence, the American Gastroenterological Association and the American College of Gastroenterology do not formally recommend the use of probiotics and prebiotics for IBS23.
Despite some promising preclinical studies, clinical evidence does not support the use of prebiotics for IBS, as they have not shown significant improvements in symptoms24,25.
Emerging dietary interventions
There is no available information on the effect of intermittent fasting in patients with IBS. However, a small study with 21 healthy Muslim individuals who practiced Ramadan (a model of intermittent fasting) evaluated the effects on GI motility26. The study concluded that all subjects showed a decrease in weight, body mass index, and waist circumference and with a reduction in subcutaneous and visceral fat, and insulin resistance. After fasting, hydrogen breath tests showed an increase in carbohydrate fermentation and a faster orocecal transit25. Further studies, especially in humans and in the context of disease, are needed to determine its efficacy and mechanism of action in IBS.
Nutritional assessment tools in irritable bowel syndrome
Since IBS presents as diarrhea-predominant, constipation-predominant, or mixed subtypes, it is essential to identify triggers to guide dietary management. The main tool that can be useful in identifying triggers is a food diary or log, in which the patient is asked to monitor and record foods consumed prior to the onset of symptoms to correlate them. Figure 1 illustrates an example of a log format that the patient can complete. Other options include:
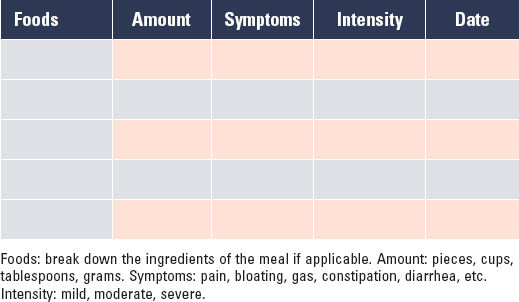
Figure 1. Example of a food diary as an assessment tool.
- – Bowel movement diary: frequency and appearance of stools are recorded using the Bristol Stool Scale.
- – 24-hour recall: assesses all foods consumed the previous day (or a typical day) and allows identification of whether the patient consumes enough fruits and vegetables, whether there is excess intake of processed foods, or if the diet is high in fat, among other aspects.
Patient monitoring should always be carried out by a qualified nutritionist, who can recognize the types of foods and quantities to which the patient may be hypersensitive, and advise on appropriate substitutions. These methods, focused on adapting and personalizing treatment for each individual, reduce the risk of nutritional deficiencies and improve adherence.
Challenges and controversies surrounding dietary interventions
Tuck et al4. evaluated responses during each phase of the low-FODMAP diet in 80 patients, observing that 78% adhered during phase 1 (restriction), but adherence decreased by 30% in phase 2 (reintroduction) and by an additional 8% in phase 3 (personalization), resulting in only 40% following all 3 phases adequately. For this reason, an alternative, less restrictive, history-based approach called Bottom-up has been proposed. In this approach, only 1 or 2 specific FODMAP subgroups are initially restricted, the symptomatic response is evaluated, and restrictions are continued only if necessary. It is suggested to begin with fructans, mannitol, and galactooligosaccharides, as these FODMAP subgroups are most frequently reported as triggers (Fig. 2)5.
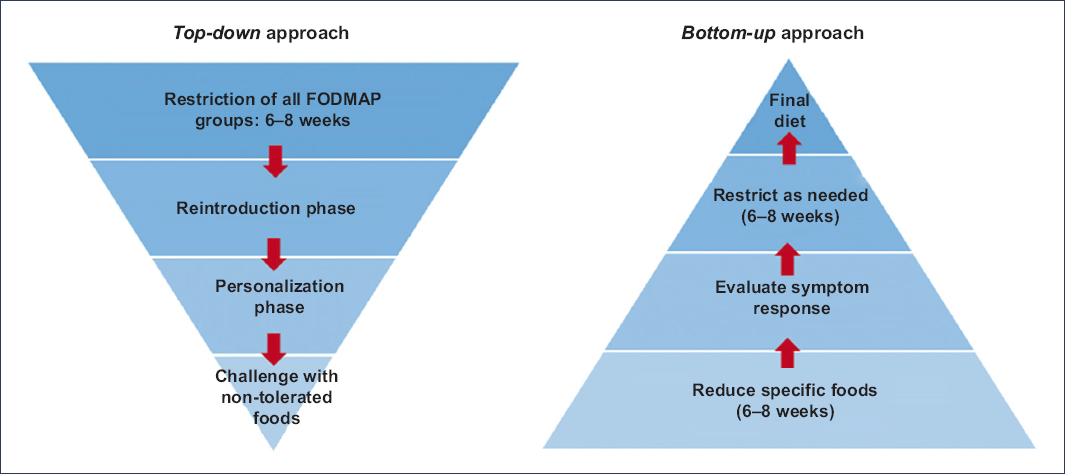
Figure 2. Alternative bottom-up approach to the traditional low-FODMAP diet.13
Although this approach has not been well studied, the Bottom-up strategy requires a thorough assessment of the patient’s dietary habits to identify likely triggers. For example, if the patient uses artificial sweeteners (in coffee, sodas, or sugar-free drinks, or if they chew gum or consume sugar-free mints, candies, or chocolates) or consumes large amounts of fruit or fruit juices, restricting excess fructose and polyols may yield a good response. Conversely, if the patient consumes large amounts of wheat, onion, or legumes, they may benefit from restricting fructans. Lactose intolerance must also be considered27.
After initial restriction of 1 or 2 foods or subgroups for approximately 2 weeks, symptoms are reassessed, and if they have improved, no further restrictions are needed. If symptoms persist, additional foods or subgroups can be added to the dietary restriction until symptoms resolve or lack of response is observed5,27.
Possible risks of prolonged restrictive diets
An important factor to consider when recommending restrictive or elimination diets is the risk of eating disorders, specifically orthorexia nervosa. Some signs and symptoms reported in the literature include compulsively checking nutrition labels, avoiding many food groups, being unable to eat anything that does not appear clean or healthy, and feeling stress related to food.
A particular disorder increasingly observed in IBS patients is avoidant/restrictive food intake disorder (ARFID). This differs from anorexia nervosa in that there is no preoccupation with weight.
Very little literature exists on ARFID in gastroenterology, but it may be more common than clinicians realize. Dr. Chey’s group in Michigan reported that of more than 300 patients seen in motility and brain-gut clinics, 20% screened positive for ARFID28.
For this reason, it is important to monitor and avoid extreme or unnecessary dietary restrictions, which may place patients at risk of long-term nutritional deficiencies.
Personalized diet or general guidelines?
In conclusion, there is no standardized diet that will work for all IBS patients. Therefore, a personalized diet adapted to each patient’s lifestyle, preferences, beliefs, and socioeconomic status is recommended.
Patients must be reminded and educated that tolerance will largely depend on the amounts consumed and the combinations with other foods. Using a food diary when symptoms occur is advisable, as it allows appropriate adjustments based on recorded information.
Funding
The author declared not having received any funding for this study.
Conflicts of interest
The author declared no conflicts of interest whatsoever.
Ethical considerations
Protection of humans and animals. The author declares that no experiments on humans or animals were conducted for this study.
Confidentiality, informed consent, and ethical approval. The study does not involve patient personal data and does not require ethical approval. The SAGER guidelines do not apply.
Declaration on the use of artificial intelligence. The author declares that no generative artificial intelligence was used in the preparation of this manuscript.
