Introduction
Upper gastrointestinal endoscopy is considered the reference method for the diagnosis of peptic ulcer disease. Endoscopy, in addition to directly visualizing ulcers, allows biopsies to be taken and complications to be treated.1,2
Taking biopsies is essential to rule out ulcers of malignant etiology in the stomach. Gastric biopsies are also part of the protocol for searching for Helicobacter pylori.1
Compared to double-contrast barium testing, endoscopy is significantly more sensitive (92 vs. 54%) and specific (100 vs. 91%) for the diagnosis of ulcers, which is why the use of this imaging technique has decreased when diagnosing peptic ulcer is of interest.1
In the context of peptic ulcer disease, endoscopy is indicated when there is upper gastrointestinal bleeding manifested by hematemesis or melena, or when there is persistent vomiting that could be caused by peptic stricture (Fig. 1). Endoscopy, however, is not indicated in the case of an acute abdomen with suspected perforation due to peptic ulcer.
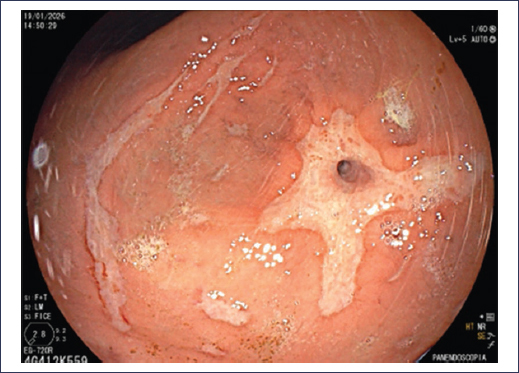
Figure 1. Pyloric stricture due to peptic ulcer.
If the symptoms are dyspepsia, international guidelines and consensus statements only recommend performing endoscopy in patients over a certain age, according to regional epidemiology, in patients with alarm clinical or biochemical features, or with persistent symptoms. Guidelines do not consider that performing endoscopy is a requirement for the management of dyspepsia in patients who come for their initial treatment with the primary care physician or gastroenterologist.3 This recommendation is based on the fact that the prevalence of dyspepsia is high and contrasts with the low frequency of endoscopic findings, with 85% of endoscopies being completely normal.4
Diagnosis of Helicobacter pylori
It is considered that 90-95% of duodenal ulcers and 50-80% of gastric ulcers are associated with H. pylori infection. It has been demonstrated that bacterial eradication treatment significantly decreases ulcer recurrence. Therefore, it is essential, in addition to having made the diagnosis of peptic ulcer, to establish whether H. pylori is present and in such case provide treatment.1,5
Traditionally, diagnostic methods for H. pylori have been divided into invasive, which require endoscopy, and non-invasive.
Non-invasive methods
Non-invasive methods include the urea breath test with 13C or 14C labeling, stool antigen testing, and serology. In clinical practice, the breath test is preferred due to its high sensitivity and specificity, both exceeding 95%, followed by stool antigen testing, which is also a sensitive and specific test, but its results can be influenced by the bacterial load in stool. Serological tests are useful in epidemiological studies, but are not recommended for diagnosing infection or for confirming H. pylori eradication. Recently, new techniques have appeared, such as nanoscale biosensors and microfluidic systems, which provide powerful analytical platforms for rapid and simple diagnosis using saliva or stool samples. These are methods that can be used in the office, obtaining results in minutes. However, these techniques are not yet widely disseminated.6–8
Invasive methods
Endoscopy offers multiple possibilities for the diagnosis of H. pylori. Thanks to technological advances, such as high definition, magnification, and spectral imaging, which allow detailed characterization of the gastric mucosa, recent studies suggest that endoscopy can predict the presence of H. pylori. When the Kyoto classification is used and the score obtained is > 2, the presence of H. pylori can be predicted with up to 90% accuracy. This classification also has a high negative predictive value; when the score obtained is 0, the possibility of H. pylori infection is nil.9 This, of course, requires that endoscopy be performed by expert endoscopists. In the Western world, it is considered necessary to have an accurate diagnosis of H. pylori before initiating treatment.6 Endoscopy allows samples to be taken for rapid urease testing, histological evaluation, culture, and detection of bacterial genetic material by polymerase chain reaction and fluorescence in situ hybridization. H. pylori can even be detected by direct observation of live fluorescent cells by in vivo fluorescence hybridization.6,7 Each of these methodologies has its advantages and disadvantages. Rapid urease testing is popular for its low cost and specificity of 95-100%. Like other diagnostic methods, with the exception of serology, the use of acid inhibitors can lead to false-negative results, so it is suggested to discontinue this type of drug 14 days before performing the test. The great advantage of histology, in addition to allowing direct visualization of the bacteria when stains such as hematoxylin-eosin and Giemsa are used, is that it also allows identification of precancerous conditions such as atrophy and metaplasia.6 On this particular point, the new European guidelines for the management of epithelial precancerous conditions and early gastric cancer (MAPS III) recommend that from the first diagnostic endoscopy, gastric biopsies be performed to identify the presence of H. pylori and precancerous conditions that allow risk stratification (opportunistic diagnosis).10 It is suggested that biopsies be taken according to the Sydney protocol. Culture of fresh samples taken during endoscopy has a specificity of 100%, but its sensitivity can be limited by transport logistics and the transport culture medium. It is currently used less frequently due to logistical inconveniences, combined with high costs and waiting time. Before the advent of molecular tests, culture was proposed as the method of choice when antibiotic sensitivity testing was desired in patients in whom eradication treatment had failed. The increase in H. pylori resistance to antimicrobials requires that sensitivity testing be performed more and more frequently in order to provide effective personalized treatments. Molecular genotype evaluation, through polymerase chain reaction tests and next-generation massive sequencing, allows the identification of mutations related to antibiotic resistance. They have the advantage that they can be performed from fresh samples or biopsies in formalin, and even in stool. The major drawback is cost and low availability.7,8
Endoscopy in the diagnosis of bleeding peptic ulcer (Forrest classification)
Direct visualization of ulcers allows their characterization, which is particularly important in the case of bleeding, where the presence of stigmata allows prognosis to be established and management to be directed. In this regard, the Forrest classification, described in 1974, continues to be widely used. This classification includes three main categories: I (active bleeding), II (recent bleeding), and III (ulcer with clean base). Category I is subdivided into Ia for spurting hemorrhage and Ib for oozing hemorrhage from the ulcer. Category II accepts three possibilities: IIa for visible vessel, IIb for presence of adherent clot, and IIc for flat spot at the ulcer base (Figs. 2 to 4). This classification is used to predict the risk of bleeding recurrence, need for surgery, and mortality (Table 1). International guidelines suggest that endoscopic treatment should be offered to patients with Forrest Ia, Ib, and IIa ulcers. In the case of ulcers with adherent clot (IIb), it is suggested to remove the clot and provide treatment if bleeding occurs or a visible vessel is found.11,12
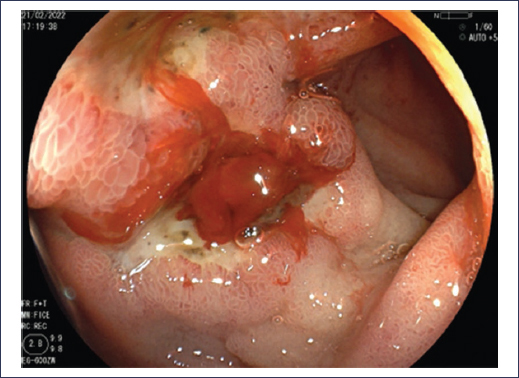
Figure 2. Duodenal ulcer Forrest Ib.
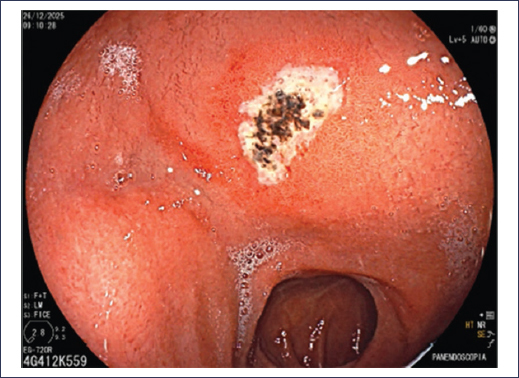
Figure 3. Duodenal ulcer Forrest IIc.

Figure 4. Gastric ulcer Forrest III.
Table 1. Bleeding stigmata and average rates of continued bleeding, need for surgery, and mortality
| Stigma | Continued bleeding | Need for surgery | Mortality |
|---|---|---|---|
| Active bleeding | 55% (17-100%) | 35% (20-69%) | 11% (0-23%) |
| Visible vessel without bleeding | 43% (0-81%) | 34% (0-56%) | 11% (0-21%) |
| Adherent clot | 22% (14-36%) | 10% (5-12%) | 7% (0-10%) |
| Flat spot | 10% (0-13%) | 6% (0-10%) | 3% (0-10%) |
| Clean base | 5% (0-10%) | 0.5% (0-3%) | 2% (0-3%) |
|
Adapted from Laine and Jensen11. |
|||
One of the main concerns with the Forrest classification is the significant intra- and interobserver variability. For several years, an endoscopic Doppler ultrasound probe has been studied that is introduced through the working channel of a conventional endoscope. This probe provides an objective evaluation of the peptic ulcer in terms of blood flow: if the Doppler signal is positive, it indicates that there is an invisible vessel below the surface. The Doppler probe can be used to determine whether endoscopic therapy is necessary even if high-risk stigmata are not visualized, as well as to determine whether endoscopic therapy was adequate to interrupt blood flow. A meta-analysis of eight studies showed that the Doppler ultrasound probe is a useful tool for the management of bleeding ulcers and adds valuable information to visual assessment.13
With the aim of avoiding incorrect Forrest classifications, a study used artificial intelligence to create a real-time convolutional neural network that allows evaluation of the Forrest classification in the context of bleeding peptic ulcers. The results showed that this technique was even more accurate than the evaluation performed by expert endoscopists.14
Other diagnostic methods in peptic ulcer disease
Capsule endoscopy
Capsule endoscopy is a first-line diagnostic method for evaluation of the small bowel. Considering that not all peptic lesions require endoscopic treatment, it has been proposed that capsule endoscopy could play a role in acute upper gastrointestinal bleeding as a risk stratification tool. The MiroCam Navi capsule (Intromedic Ltd, Seoul, Korea) can be moved in the gastric cavity by a portable external magnet (MACE, magnetically assisted capsule endoscopy). Real-time images are displayed on a monitor and video recording can be viewed at the end of the examination. The capsule has an 11-hour battery life, which allows subsequent passive exploration of the small intestine in the same session. A recent study with a limited number of patients showed that MACE detects more upper gastrointestinal lesions than endoscopy, although there were no statistically significant differences. MACE appears to be comparable to endoscopy for the detection of lesions suspected of being the cause of bleeding.15 In that study, capsule endoscopy was well tolerated and allowed prediction of safe early discharge. MACE also detected small bowel bleeding in 18% of the cohort. More studies are required to determine whether MACE could play a role in upper gastrointestinal bleeding, either as a diagnostic alternative to endoscopy, locating the bleeding site and stratifying high- and low-risk patients, to avoid admission of those without risk stigmata and prioritizing patients with stigmata for early endoscopy.15
Computed tomography
Computed tomography (CT) is an indispensable resource in the emergency department. Currently, CT is a fundamental diagnostic tool in patients who arrive at the emergency department with abdominal pain. In the context of perforated peptic ulcer, CT is very useful since it allows free air to be identified in the abdominal cavity, regardless of whether it is not possible to demonstrate the site of perforation. However, in a large proportion of CTs requested in the emergency department, an acute abdomen is not identified. Could CT detect peptic ulcer disease? In general, it is considered that tomographic findings are nonspecific for the diagnosis of ulcer. In a retrospective study that included 51 patients with a diagnosis of peptic ulcer by endoscopy, two radiologists evaluated contrast-enhanced CTs performed within 24 hours prior to endoscopic diagnosis and the results showed, first, that agreement between both radiologists was very high.16 The findings that consistently suggested the presence of ulcer were high-density gastric content, focal low-attenuation wall thickening, and focal luminal outpouching.16 More studies are needed to validate these tomographic findings that allow suspicion of a peptic ulcer on CT for referral to endoscopic procedure.
Funding
The authors declare that they have not received funding for this study.
Conflicts of interest
The authors declare that they have no conflicts of interest.
Ethical considerations
Protection of human and animal subjects. The authors declare that no experiments were conducted on human beings or animals for this research.
Confidentiality, informed consent, and ethical approval. The study does not involve personal data, clinical histories, or human biological samples, therefore it does not require ethical approval. SAGER guidelines do not apply.
Declaration on the use of artificial intelligence. The authors declare that no type of generative artificial intelligence was used for the writing or creation of content in this manuscript.
