Introduction
Gastroesophageal reflux disease (GERD) is defined as a condition that develops when reflux of gastroduodenal contents into the esophagus causes troublesome symptoms or complications. The term “troublesome” refers to symptoms that interfere with the patient’s well-being and negatively affect quality of life1. This definition recognizes that GERD is not limited to the presence of endoscopic lesions (erosive GERD), but can also manifest as non-erosive GERD or with extraesophageal symptoms (chronic cough, laryngitis, asthma, or non-cardiac chest pain). Additionally, it considers the possibility of long-term complications, such as esophageal stricture or Barrett’s esophagus, highlighting that diagnosis can be based on both clinical presentation and objective confirmation through functional or endoscopic tests.
The most modern definition is proposed by the Lyon Consensus 2.0 (2022), which introduces the concept of “actionable” GERD, that is, one in which there is sufficient objective evidence to justify targeted therapeutic intervention, such as esophageal acid exposure > 6% of total time on pH-metry or pH-impedance monitoring, severe erosive esophagitis (Los Angeles C/D), peptic stricture, or Barrett’s esophagus. When findings fall within an intermediate range (4-6% acid exposure), diagnosis requires correlation with other markers, such as symptom-reflux association, the number of reflux episodes, or baseline esophageal impedance. This approach not only classifies GERD as erosive, non-erosive, or with extraesophageal manifestations, but also more precisely guides when to initiate, intensify, or even reconsider treatment, optimizing clinical decision-making1,2.
Having a global consensus definition for the disease is essential, as it facilitates clinical management and enable collaborative research to help patients, physicians, and regulatory agencies alike.
Epidemiology
Global
The true prevalence of GERD is difficult to estimate, as generally the prevalence of indicative symptoms is reported rather than the fully confirmed disease, and it depends on the criteria used for diagnosis. A systematic review with meta-analysis on the prevalence and risk factors of GERD estimated a combined global prevalence of 13.98%, with marked variability between regions and countries. Figures ranged from 4.16% in China to 22.40% in Turkey, and in our region, from 12.88% in Latin America and the Caribbean to 19.55% in North America3. Based on these data, it is estimated that approximately 1,030 million people worldwide are affected by GERD (Fig. 1).
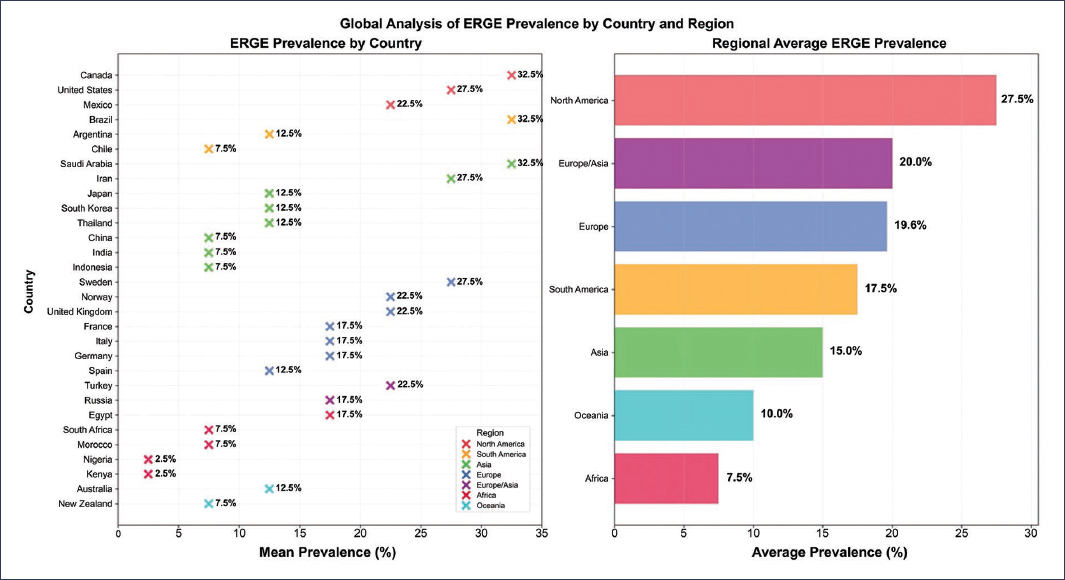
Figure 1. Global analysis of GERD prevalence by country and region.
In another meta-analysis that included 102 population-based studies with 460,984 participants from various countries, marked geographic variability in the prevalence of gastroesophageal reflux symptoms was observed, ranging from 2.5% in China to 51.2% in Greece. Using standardized criteria of weekly frequency of heartburn or regurgitation, the pooled global prevalence was 13.3% (95% confidence interval [CI]: 12.0-14.6). The analysis identified significant but modest risk factors, including age ≥ 50 years (odds ratio [OR]: 1.32), smoking (OR: 1.26), use of aspirin or other non-steroidal anti-inflammatory drugs (OR: 1.44), and obesity (OR: 1.73), with the latter showing the strongest association4.
Regarding sex, slight differences in prevalence have been reported: 16.7% in women and 15.4% in men4. However, different studies have reported that erosive reflux disease predominates in men, with a ratio of 1.5:1, compared to the non-erosive phenotype, which predominates in women. This is associated with the role played by steroid hormones as modulators of the immune system, as estrogen has anti-inflammatory activity by reducing migration, adhesion, and production of chemical mediators5. Estrogen has been shown to attenuate reflux esophagitis through inactivation of mast cells by inhibiting cytokine production, which are primarily involved in initiating tissue damage induced by reflux esophagitis. It was also revealed that estrogen significantly suppressed the level of macrophage inhibitory factor in esophageal tissue, which regulates inflammation and the innate immune response involved in macrophage infiltration and tumor necrosis factor-alpha production5.
When comparing other aspects, such as economic status, a higher frequency of disease symptoms is reported in social classes considered middle-upper and upper. When considering a person’s occupation, it is more frequent in professionals compared to homemakers, students, unemployed individuals, and retirees. Regarding education, a gradual increase was noted as it advances, mainly affecting subjects with university education2.
Another way to report the actual increase in GERD cases worldwide is through the rise in its complications, especially esophageal adenocarcinoma. For example, the number of new reported cases of Barrett’s esophagus was documented in different studies at 11 per 100,000 patients in the 1990s and up to 23 per 100,000 patients in the 2000s. In the case of esophageal adenocarcinoma, a doubling of incidence from 1976 to 1987 and an up to sevenfold increase by 2010 were reported5.
Mexico
The epidemiological characterization of GERD in Mexico has been supported by several relevant studies. López-Colombo et al.6 evaluated 500 people from the general population in Tlaxcala using the Rome II questionnaire and found heartburn in 19.6% (95% CI: 16.2-23.4). Subsequently, Schmulson7 studied 40 patients seen in a private practice in Mexico City, applying the same questionnaire and complementing the evaluation with endoscopy in 36 cases and esophageal pH-metry using Bravo capsule in the remainder. The mean age was 44.5 ± 2.5 years, predominantly female (62.5%) and with an average body mass index of 25.5 ± 0.8 kg/m2. Heartburn was reported in 40% of participants, with GERD confirmed by endoscopy in 62.5% of them, whereas among those asymptomatic according to the questionnaire, endoscopy and pH-metry detected the disease in 29.2%. A third study, conducted by Peralta-Pedrero et al.8, applied the Carlsson-Dent questionnaire to 400 adults over 60 years of age at the first level of institutional care, and identifying GERD in 25% (95% CI: 21-29).
Years later, the largest study in the country, the national SIGAME survey, evaluated an open population (nearly 4,000 subjects from throughout the Mexican Republic) applying Rome III criteria9. The results showed that heartburn or regurgitation occurred daily in 1.2% of the population, at least once a week in 12.1%, and at least once a month in 49.1%, confirming that GERD is highly prevalent in Mexico. Heartburn was most common in the mornings (62%), with very mild or mild intensity in 45.3% of cases. Regurgitation, also reported mainly in the morning (52.3%), presented very mild or mild intensity in 73.6%. Among associated symptoms, considering their occurrence at least one day per week, nausea was the most frequent (16.9%), followed by chest pain (15.3%) and vomiting (4.05%).
Regarding geographic variability, even within our country, there are differences by zone, with higher symptom frequency reported in the south-central and western regions, compared to lower frequency in the north-central and northeastern regions9 (Fig. 2).
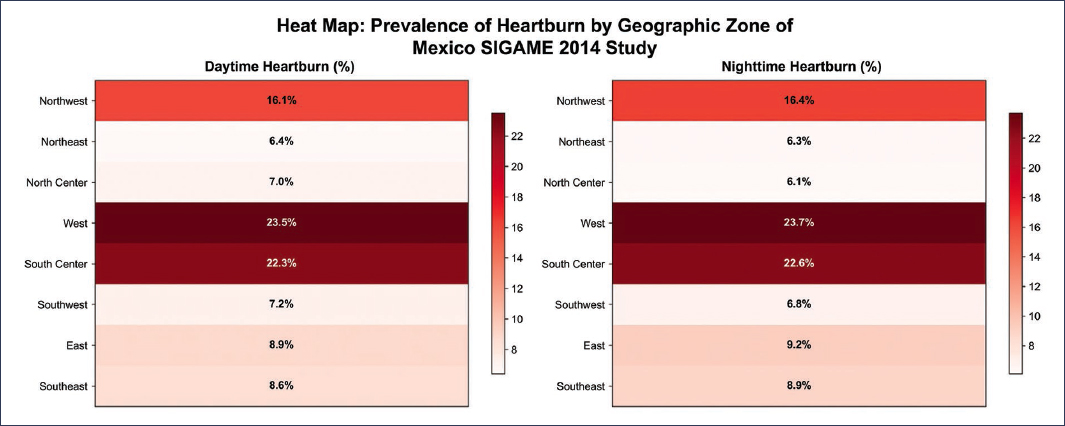
Figure 2. Heat map: Prevalence of heartburn by geographic zone of Mexico. SIGAME Study 2014.
In addition to the observed difference in prevalence by region, differences are also seen both by age and sex. Subjects over 50 years old report a prevalence of 17.3% and those under 50 years old 14%10. The SIGAME study confirms in our country that individuals with disease symptoms were older than those without the disease (average age 42.6 years vs. 37.8 years; p = 0.0001)9. The mechanisms explaining the increase in prevalence with age include alterations in esophageal motility, decreased saliva and bicarbonate secretion, reduced lower esophageal sphincter (LES) pressure, diaphragmatic weakness, and increased incidence of hiatal hernia, the presence of comorbidity, and concomitant use of drugs such as nitrates, anticholinergics, calcium channel blockers, benzodiazepines, and antidepressants, which can decrease LES pressure and increase disease incidence11.
Risk factors
GERD is a multifactorial condition in which the interaction of individual predisposition, lifestyle habits, and comorbidity influences its onset and severity. Among the most recognized risk factors are obesity, pregnancy, smoking, excessive consumption of alcohol, coffee, or fatty foods, and the use of drugs that decrease LES pressure (Table 1). Anatomical and functional conditions, such as hiatal hernia, delayed gastric emptying, and alterations in esophageal motility, have also been identified, facilitating the reflux of gastric contents. Genetic factors and psychological stress can act as modulators, increasing susceptibility or the intensity of symptoms.
Table 1. Risk factors and their relationship with gastroesophageal reflux disease
| Risk factor | Mechanisms involved |
|---|---|
| Obesity | Decreased LES pressure |
| Increased transient LES relaxations | |
| Increased intra-abdominal pressure | |
| Hiatal hernia | |
| Smoking | Decreased LES pressure |
| High-fat diet | Decreased LES pressure |
| Delayed gastric emptying | |
| Coffee, tea, chocolate | Decreased LES pressure |
| Decreased intraesophageal pH | |
| Carbonated beverages | Decreased LES pressure |
| Increased transient LES relaxations | |
| Decreased intraesophageal pH | |
| Alcohol | Direct damage to esophageal mucosa |
| LES dysfunction | |
| Motility disorder | |
| Helicobacter pylori | Reduction of GERD complications |
| Decreased acid production | |
| Physical activity | Regular moderate-intensity exercise (150 min per week) is protective |
| Genetics | Concordance rate of 42% in monozygotic twins vs. 26% in dizygotic twins |
| Dysbiosis | Proteobacteria, Firmicutes, Bacteroidetes, Fusobacteria, and Actinobacteria have greater relevance for esophageal disorders |
LES: lower esophageal sphincter; GERD: gastroesophageal reflux disease.
Obesity
Among the risk factors with the greatest impact is obesity, as an increase in disease prevalence of up to 22.1% (OR: 1.73) has been documented compared to subjects without obesity, with a prevalence of 14.2%4. However, waist circumference, as well as waist-to-hip ratio, are considered to have better correlation with disease symptoms and complications (erosive esophagitis, Barrett’s esophagus, and esophageal adenocarcinoma) than body mass index. Reports relate central adiposity with a risk of erosive esophagitis of 1.87, Barrett’s esophagus of 1.98, and esophageal adenocarcinoma of 2.5112.
Numerous mechanisms have been described by which individuals with obesity have greater acid exposure, among which stand out a hypotensive LES, an increase in transient LES relaxations, and an increase in intra-abdominal pressure with development of hiatal hernia12. The commonly suggested pathway is that increased abdominal pressure relaxes the LES, thereby exposing the esophageal mucosa to gastric contents. This is associated with visceral fat being metabolically active and related to serum levels of adipokines such as interleukin-6 and tumor necrosis factor-alpha, which influence the disease and its complications, such as carcinogenesis13.
Results from 24-hour pH monitoring have demonstrated that obesity is associated with a significant increase in the number of both reflux episodes and long-duration episodes, especially during the postprandial period12. Similarly, monitoring by pH-impedance metry reports not only an increase in acid reflux episodes but also in non-acid reflux episodes. Using high-resolution esophageal manometry, the morphology and function of the esophagogastric junction have been evaluated, and a clear correlation has been reported between alterations in both intragastric and gastroesophageal pressure gradients and waist circumference, which promotes retrograde flow of gastric contents into the esophagus12. Another finding was the correlation of body mass index and waist circumference with axial separation of the LES from the diaphragmatic crura due to increased intragastric pressure12,13. This is relevant, as the presence of hiatal hernia has pathophysiological implications in the pathogenesis of the disease, such as reduced LES pressure, impaired esophageal acid clearance, and greater sensitivity to transient LES relaxations induced by distension.
Smoking
Regarding smoking, a GERD prevalence of 19.6% (OR: 1.26) is reported in smokers compared to 15.9% in non-smokers3, and it is described that there is even up to a threefold decrease in regurgitation and heartburn symptoms upon cessation of this habit. Furthermore, it has been documented that the duration of smoking is related to alterations in esophageal motility and emptying14; as tobacco reduces resting LES pressure. Studies have demonstrated that in healthy subjects, tobacco reduced LES pressure by 37% in 2-3 minutes, while inhaling an unlit cigarette induced no change in LES pressure15. Sphincter pressure remained low until smoking was stopped and then returned to normal. Another study obtained similar results, observing that smoking cigarettes caused a decrease in LES pressure of 41% in 1-4 minutes16, and returned to normal in 3-8 minutes after stopping smoking16. Similarly, pH measurements also showed an increase in reflux during and after smoking. The probable mechanism by which LES pressure is reduced is the blockade of cholinergic receptors by nicotine and the consequent relaxation of circular muscle fibers. Cigarette consumption was also associated with prolonged acid clearance time, due to decreased salivary secretion and lower bicarbonate concentration14.
Diet
Diet, especially high consumption of fats, sugar, chocolate, and salt, as well as decreased consumption of fruits and vegetables, has been associated with the disease, but the evidence is contradictory. Some studies report an increase in symptoms with consumption of a high-fat diet and a reduction with a high-fiber diet. Conversely, in studies conducted on monozygotic twins, they are not related to the disease17.
The relationship between fat intake and GERD has been attributed to decreased basal LES pressure when consuming such foods. However, it is known that meals rich in fats release high amounts of cholecystokinin, which delays gastric emptying by reducing antral contractions, increasing pyloric pressure and promoting fundic relaxation, resulting in gastric distension, a trigger for transient LES relaxations18.
Consumption of a high-fiber diet has been inversely associated with the risk of reflux symptoms. Studies have shown that consumption of bread with high dietary fiber content reduces reflux risk by half compared to consumption of white bread with low fiber content19,20. One explanation for this is that dietary fiber removes nitrites in the stomach, which would reduce nitric oxide formation and, consequently, LES relaxation. A Mediterranean diet, characterized by high consumption of fruits, vegetables, legumes, whole grains, fish, and olive oil, as well as moderate consumption of alcohol and dairy, and low amounts of red meat and processed products, is associated with a decrease in the frequency of reflux symptoms19.
Coffee and tea consumption has been related to symptom frequency; however, the mechanism involved is not completely understood. Studies with healthy subjects have demonstrated that intragastric administration of these substances causes a significant decrease in LES pressure and pH in the lower esophagus, effects not observed with decaffeinated coffee18. However, a systematic review shows that the evidence is particularly contradictory, as several studies found no increased risk of reflux symptoms in coffee consumers21. Regarding carbonated beverages, they have been shown to decrease LES pressure and increase the number of transient relaxations18. Similarly, it has been documented that they cause a short-term reduction in intraesophageal pH and increase gastric acid secretion10.
Alcohol consumption is a clear factor associated with GERD, as an increase in symptoms of up to 20.3% is reported, compared to 18.1% in non-consumers3. Among the mechanisms are direct damage to both the esophageal mucosa and esophageal function, causing LES dysfunction, abnormal peristalsis, and motility disorders. Alcohol can increase the aggressiveness of refluxed gastric content by influencing gastric acid secretion, although it depends on the type of alcohol administered. For example, pure ethanol does not stimulate gastrin secretion, whereas beer and wine do18. In a study with healthy subjects without GERD, white wine was associated with both a reduction in LES pressure and an increase in time with esophageal pH < 4, whereas not red wine, which did induce disease symptoms but did not increase time with pH < 4 despite having a higher alcohol percentage than white wine (12% vs. 8%)22. These findings suggest that other ingredients, rather than alcohol, promote reflux among consumers of these alcoholic beverages14. However, other studies report an inverse relationship between alcohol consumption and reflux, documenting that subjects with heavy alcohol consumption have less symptom prevalence than non-drinkers (49% vs. 56%, respectively)23. Among the hypotheses mentioned is that subjects with heavy alcohol consumption have fewer heartburn episodes, probably secondary to a reduction in symptom perception induced by neuropathy18.
Chocolate is another substance that has been related to exacerbation of reflux symptoms. Studies have concluded that its intake significantly reduces LES pressure from 14.6 ± 1.1 to 7.9 ± 1.3 mmHg24. Similarly, other studies have demonstrated a significant increase in acid exposure during the first hours after consumption18.
Capsaicin is the active compound in red pepper and spicy foods. Its importance lies in the fact that its transient receptor potential vanilloid 1 receptor is a mediator of stomach acidity. However, receptor exposure to capsaicin is characterized by its activation, followed by desensitization with chronic administration. Additionally, changes in LES pressure and gastric emptying appear to be dose-dependent, so patients could develop heartburn, but probably not induced by increased gastroesophageal reflux18.
Some other foods have also demonstrated association with disease symptoms. For example, consumption of food with high salt content increases the risk of reflux by up to 70% compared to subjects who do not add extra salt to their food (OR: 1.7); onions increase both the number of reflux episodes and the percentage of time with pH < 4, heartburn, and belching during the first 2 hours after consumption; regular milk causes more heartburn episodes than low-fat milk; and citrus fruits have been correlated with heartburn, but the mechanism involved is unknown18.
Since many reflux symptoms occur in the postprandial period, not only foods associated with reflux symptoms have been studied but also dietary practices, such as rapid food intake, irregular meal patterns, and even skipping meals or eating shortly before bedtime20. It has been shown that subjects with a “moderate to fast eating pace” are more likely to have GERD compared to those with a “moderate eating pace.” Similarly, GERD prevalence is higher in subjects with an “irregular meal pattern” than in those with a “regular meal pattern,” and subjects with a “short interval between meals and sleep” are more likely to suffer from GERD than those with a “long interval between meals and sleep.” Other studies have reported that patients who lie down within 3 hours after food intake have an OR of 7.45 for GERD development, compared to subjects who lie down more than 4 hours later25.
Physical activity
Regular moderate-intensity aerobic physical activity is inversely associated with disease symptoms26, unlike strenuous exercise, which has been positively associated with the disease17. Clark et al.27 reported that running was associated with higher reflux prevalence, while cycling was associated with lower incidence, suggesting that low-intensity aerobic exercises, such as walking, cycling, and yoga, may offer protective benefits. It has been reported that people who perform 150 minutes of physical activity per week experience a 72% reduction in the risk of developing GERD26.
Genetics
Genetic factors were first related to GERD etiology by twin studies, which reported significantly higher concordance rates in monozygotic twins, up to 42%, compared to 26% in dizygotic twins, with an estimated heritability of 43%28. The most successful genetic study has been the genome-wide association study (GWAS), with large sample size being a key feature in successful studies; however, initial GWAS for GERD did not identify any risk genes, whereas more recent approaches using a broad phenotype definition to maximize sample size succeeded in identifying 25 risk loci29. Similarly, strong genetic relationships were revealed between the disease and various traits, among which depression stands out, probably reflecting the psychological component previously demonstrated as associated, as well as obesity, an expected finding given that overweight is an important risk factor for the disease29.
Regarding GERD complications, their association with Barrett’s esophagus and esophageal adenocarcinoma is well known, in which observational family studies report that they have a shared genetic basis, as the risk of all three diseases increases when a family member is affected by any of them. Gharahkhani et al.30 estimated the degree of shared genetic background among these three diseases, reporting a significant genetic overlap of 77% between GERD and Barrett’s esophagus, and 88% between GERD and esophageal adenocarcinoma. Likewise, a GWAS meta-analysis involving information from more than 10,000 patients identified new risk genes and biological pathways representing pathophysiological mechanisms for these diseases31. Among the strongest associations was the CFTR gene on chromosome 7q31. This gene encodes an ATP-binding cassette membrane protein that functions as a chloride channel and is mutated in cystic fibrosis, a disease in which up to 81% of patients show reflux symptoms, in addition to an increased risk of esophagogastric junction cancer32.
Dysbiosis
In recent years, the correlation between the occurrence and progression of various intestinal diseases and the intestinal microbiota has been clarified. Dysbiosis has been related to the development of visceral hypersensitivity, suggesting the possible involvement of microbiota dysregulation in the pathogenesis of GERD-related diseases33. The study of esophageal microbiota aims to establish the relationship between pathogenesis, early detection, and therapeutic approaches for esophageal disorders. It has been noted that the composition of esophageal microflora varies between GERD esophagi and normal esophagi. Some differences are greater colonization by gram-negative microorganisms, particularly Campylobacter, in the esophageal mucosa of GERD patients compared to healthy individuals28.
The Clostridiales Vadin BB60 family group, the Lachnospiraceae UCG004 genus, the Methanobrevibacter genus, and the Actinobacteria phylum have shown an inverse correlation with disease vulnerability. Likewise, they are considered contributors to short-chain fatty acid biosynthesis, which not only serve as the main energy source for colonocytes but also play a fundamental role in bidirectional regulation of colonic motility, preservation of intestinal homeostasis, and improvement of intestinal barrier integrity. The Clostridiales group has been related to esophageal pathologies such as esophagitis and Barrett’s esophagus, as it influences inflammatory processes of the esophageal mucosa and contributes to the development of intestinal metaplasia. A Japanese study using quantitative polymerase chain reaction of the 16S rRNA gene reported that the Proteobacteria, Firmicutes, Bacteroidetes, Fusobacteria, and Actinobacteria groups have greater relevance for esophageal disorders than absolute bacterial counts29. On the other hand, the Mollicutes class, the Anaerostipes genus, and the Tenericutes phylum have shown association with GERD risk. For all the above, different probiotic strains have been studied, among which Lactobacilli spp. and Bifidobacteria spp. have demonstrated efficacy in GERD relief33.
Socioeconomic and quality of life impact
Due to its high prevalence, chronicity of symptoms, and effect on quality of life, the economic impact of GERD is usually very high. A significant number of patients consume medications that inhibit gastric acid secretion, either by physician indication or by self-prescription. In the late 1990s, US statistics reported a direct disease cost of 9.3 billion dollars, of which 63% corresponded to medications, 27% to hospitalizations, 7% to consultations, 2% to home visits, and 1% to emergency care34. In the 2000s, proton pump inhibitor sales reached 10 billion dollars, representing two of the five best-selling drugs nationally and 50.7% of prescriptions for digestive system diseases, equivalent to 77.3% of total costs35. To this are added indirect costs, such as days of absence for medical consultations, appointments for study performance, and decreased productivity during the workday. Overall, a 41% decrease in productivity is calculated, with an average cost of $237.00 over a 3-month period and an economic impact of $3,441.00 total cost for the disease, compared to healthy subjects2. In other countries, such as the United Kingdom, estimated expenses of both medical care and work absenteeism due to GERD are calculated at 760 million pounds sterling, and in Germany, the direct cost per patient per year was approximately 342 euros36. Additionally, patients with refractory disease have even more economic impact, with reported differences of $26,057 versus $15,285 per patient per year.
Furthermore, expenses related to antireflux surgery should not be overlooked, with estimated direct medical care costs per patient were $5,170 in outpatient care and $15,108 in hospitalized patients, accumulating up to $29,513 if an additional surgical procedure is required37.
GERD significantly affects the quality of life of subjects who suffer from it. Different questionnaires report a reduction in quality of life similar to that of patients with chronic degenerative diseases such as diabetes mellitus, arterial hypertension, or arthritis14. A significant percentage of patients must drastically modify their eating habits, up to 60% experience sleep-related problems, and 40% report difficulty concentrating at work due to symptoms. Indicators of daily activity, difficulty dressing, diet, personal relationships, and psychological well-being have been shown to be affected, all with statistical significance, in subjects reporting heartburn at least one day per month in our country, compared to healthy subjects. Worldwide, GERD accounted for 3.6 million years lived with disability in the 1990s, reflecting the frequency and non-fatal health consequences of a disease that represents 0.6% of all years lived with disability, which increased by 77.19%, equivalent to 6 million for 201738.
Studies on the quality of life of GERD patients based on questionnaires such as GERD-HRQoL report that approximately 83.3% have poor quality of life due to the disease, while only 16.7% have good quality of life30. The symptom that most frequently affects patients is heartburn, up to 85.9%, both after meals and when lying down. In contrast, the least reported symptoms are dietary changes (61%) and sleep disturbances due to acidity (44%)39.
Conclusion
GERD constitutes a global health problem, with significant prevalence and marked geographic variability, influenced by genetic, anatomical, functional, and lifestyle factors. Its impact extends beyond symptomatology, as it significantly affects quality of life, work productivity, and places a burden on health systems due to its direct and indirect costs.
The diagnostic approach should be based on updated criteria, such as those proposed by the Lyon Consensus 2.0, which facilitate optimization of therapeutic decision-making. Treatment requires a comprehensive and individualized approach that combines lifestyle modifications, pharmacotherapy, and, in selected cases, surgical interventions or emerging therapies.
Future research should focus on identifying subpopulations with differentiated risk, evaluating innovative interventions, and understanding the role of microbiota and genetics in disease pathophysiology, aiming to improve prevention, diagnosis, and treatment.
Funding
The authors declare that they received no funding for this study.
Conflicts of interest
L. Bolio-Lavalle has no conflict of interest. J.M. Remes-Troche is an advisory board member for Adium, Bicodex, Prometis Pharma, and Carnot, and has been a speaker for Adium, Alfasigma, Carnot, Menarini Central America, and M8.
Ethical considerations
Protection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this research.
Confidentiality, informed consent, and ethical approval. The study does not involve patient personal data nor requires ethical approval. SAGER guidelines do not apply.
Declaration on the use of artificial intelligence. The authors declare that they did not use any type of generative artificial intelligence for writing this manuscript.
