Introduction
In the recommendations for good clinical practice of the Mexican Association of Gastroenterology, it is established that all patients with gastroesophageal reflux disease (GERD) should lose weight if overweight or obese, avoid smoking, and not consume those foods they identify as inducers of their symptoms. Patients with nocturnal reflux should eat dinner early, elevate the head of the bed, or sleep in the left lateral decubitus position1,2.
Lifestyle changes
Dietary modifications
Although dietary modification is currently considered the first-line treatment for GERD, the role of diet in the pathogenesis and treatment of this disease is still not well understood. Several studies have shown that unhealthy eating habits or diet can be risk factors for GERD. Changes in diet composition, eating habits, and eating patterns can lead to significant improvement in GERD symptoms.
Typical GERD symptoms occur mainly after meals, when lower esophageal sphincter (LES) pressure decreases and gastric filling or distension triggers transient LES relaxations3. Eating dinner late is associated with increased acid exposure time in the supine position4,5. In an Italian questionnaire study, 85% of participants identified specific foods capable of triggering GERD symptoms, especially spicy or fried foods, tomato, and chocolate6. The spicy components and malic and citric acids present in tomatoes may be the cause of some of these experiences. Ingestion of a high-fat meal is associated with decreased LES pressure and increased reflux events, while a high-protein meal increases LES pressure7,8. Chocolate consumption is associated with greater esophageal acid exposure9. Alcohol consumption causes a decrease in LES pressure and is associated with increased reflux10. In a prospective study involving 48,308 women, consumption of coffee, tea, or soft drinks was associated with increased risk of GERD symptoms11; conversely, a previous meta-analysis did not confirm the influence of coffee consumption12. Carbonated beverages are also associated with an increased risk of GERD symptoms, which may be due to their acidic pH and increased transient LES relaxations triggered by gastric distension13. In a mechanistic study conducted in nine patients with GERD, chronic administration of fructo-oligosaccharides increased the number of transient LES relaxations, which was associated with increased secretion of glucagon-like peptide type 114. In healthy volunteers, administration of fructans, but not fructose, increased the number of transient LES relaxations in the fourth postprandial hour, and this was accompanied by increased flatulence, suggesting an effect through colonic fermentation14.
It has been documented that certain foods, such as mint, chocolate, coffee, alcohol, and fats, can decrease LES tone, while others can exert a direct irritant effect on the esophageal mucosa, such as spicy foods and citrus fruits. Patients with GERD are usually advised to avoid fatty foods, late dinners, coffee, alcohol, carbonated beverages, and orange juice. In an Italian study, elimination of foods perceived as triggers in 100 patients with heartburn reduced symptom severity and eliminated heartburn or regurgitation in the majority8. An initial publication of a placebo-controlled crossover clinical trial in eight patients with non-erosive reflux disease reported an increase in heartburn symptoms following 6-week ingestion of capsules containing capsaicin, the active ingredient in red chili and an agonist of transient receptor potential vanilloid 1 channels15.
In a cross-sectional study with 817 participants, the Mediterranean diet (traditional composite dishes, fresh fruits and vegetables, olive oil, and fish) was associated with a statistically significant 57% decrease in GERD risk, even after adjusting for age, sex, socioeconomic factors, lifestyle, and eating habits16. Increased fiber intake (psyllium, 5 g three times daily) led to a significant increase in minimum resting LES pressure, a decrease in the number of reflux episodes, and a reduction in heartburn symptoms in a study group of 36 patients17. The current recommendation is that the diet should be individualized based on each patient’s symptoms1,2.
Eating dinner early and light
Recommendations from national and international GERD treatment guidelines recommend not eating dinner or consuming food in the 3 hours before lying down to sleep. In a study using wireless pH monitoring, it was observed that eating dinner late led to significantly longer esophageal acid exposure time and a higher number of reflux episodes compared to an early dinner. This effect was observed especially in patients with hiatal hernia, erosive esophagitis, and overweight18.
In a case-control study that included 147 patients with GERD and 294 age- and sex-matched controls without GERD symptoms, such as heartburn and regurgitation, during the last year, the time elapsed between dinner and bedtime was evaluated through a self-administered questionnaire. The authors observed that those who went to bed within 3 hours after dinner were 7.45 times more likely to experience nocturnal heartburn than those who went to bed 4 hours or more after19. In another cross-sectional study with 4,763 adults, practices related to diet were evaluated. The prevalence of GERD in the studied population was 23.5% (n = 1,120). The survey results revealed that a long interval between meal and sleep was inversely associated with GERD compared to a short interval (odds ratio [OR]: 0.73; 95% confidence interval [95% CI]: 0.57-0.95). The authors conclude that a regular eating pattern and a long interval between meals and sleep is associated with lower GERD risk20. A shorter interval between dinner and sleep is probably associated with a greater amount of food remaining in the stomach, which increases pressure on the LES in the supine position and in turn can cause reflux of gastric contents, including acid, into the esophagus.
Weight loss
The relationship between obesity and GERD development has been documented in numerous experimental and clinical studies. Increased abdominal pressure in obese patients, deficient gastric emptying, decreased LES pressure, and increased transient LES relaxations are implicated in obesity-related GERD21,22.
In a meta-analysis of eight studies in patients with GERD and obesity, which evaluated risk factors for GERD and its complications, the OR for GERD development was found to be 1.43 (95% CI: 1.158-1.734) in overweight patients (body mass index [BMI]: 25-30 kg/m²) and 1.94 (95% CI: 1.468-2.566) in obese patients (BMI > 30 kg/m²)23. In another meta-analysis, the relationship between obesity and erosive esophagitis was investigated, and it was found that being overweight (OR: 1.60; 95% CI: 1.35-1.88) or obese (OR: 2.05; 95% CI: 1.65-2.55) causes a significant increase in the risk of developing erosive esophagitis24.
Several studies have shown that weight loss leads to a decrease in the severity and duration of reflux episodes25. In a trial with 332 patients enrolled in a supervised weight control program, an average weight loss of 13 ± 7.7 kg resulted in a decrease in overall GERD prevalence from 37% to 15% (p < 0.01), with a decrease in mean GERD symptom score from 5.5 to 1.8 (p < 0.01). The authors reported an overall 81% reduction, including complete resolution of 65% of reflux symptoms, with a significant correlation between degree of weight loss and reduction in GERD symptom scores26. In a large population study conducted in Norway involving nearly 30,000 people, a BMI decrease of 3.5 or more resulted in a significant 50-70% reduction in GERD symptoms27.
Physical exercise
Several studies have reported different results on the relationship between physical activity and GERD, depending on the intensity of the activity. While excessive exercise has been shown to induce reflux, other studies suggest that there is no increase in GERD symptoms with moderate or light exercise; moreover, light and regular physical activity prevents reflux symptoms28,29. It has been suggested that excessive physical activity causes an increase in reflux symptoms by increasing transient LES relaxations30.
In a large-scale case-control study31, the authors observed that performing physical activity once a week or more, for more than 30 minutes, significantly reduced GERD risk. The authors argue that 30 minutes of physical exercise performed at least once a week reduces GERD symptoms by strengthening the crural diaphragm, which is a component of the antireflux barrier. Other authors have also shown that performing physical activity more than twice a week achieves a significant decrease in the prevalence of moderate or severe GERD symptoms (OR: 0.75; 95% CI: 0.60-0.93)32.
Abdominal or diaphragmatic breathing exercise is a simple office-based intervention that has been shown to decrease acid exposure in patients with GERD and improve quality of life. It is postulated that this intervention actively trains the diaphragmatic pillars, which contributes to LES competence and directly affects GERD severity. In a randomized clinical trial, it was shown that acid exposure decreased by almost 50% after only 4 weeks of training, which improved quality of life scores by 36% after 9 months of continuous training, and proton pump inhibitor consumption decreased by 75%. In another randomized clinical trial, the authors demonstrated that postprandial esophageal acid exposure was reduced by 56% in patients randomly assigned to diaphragmatic breathing33.
Smoking cessation has been shown to lead to a decrease in GERD symptoms, especially in individuals with normal weight. In obese patients, it did not result in a significant outcome, probably due to the more important role of obesity in the pathogenesis of GERD34.
Elevating the head of the bed and sleeping in the left lateral decubitus position
A meta-analysis of non-randomized studies revealed that elevation of the head of the bed is an effective measure to relieve reflux symptoms35. In a study, it was observed that elevation of the head of the bed reduced esophageal acid exposure and acid clearance time in 24 patients with nocturnal reflux, and produced some relief from heartburn and sleep disorders36. A study conducted in Colombia reported that elevating the head of the bed during sleep is an effective method to decrease distal esophageal reflux exposure and shorten acid clearance time, compared to a flat bed position37.
Experimental studies suggest that body position during sleep plays a role in the occurrence of reflux. The results of a study indicate that sleeping in the left lateral decubitus position can minimize nocturnal acid reflux. In a cohort study with 57 patients referred for nocturnal reflux monitoring, it was observed that the left lateral decubitus position was associated with significantly shorter esophageal acid exposure time and faster esophageal acid clearance compared to supine and right lateral decubitus positions38. Therefore, interventions aimed at promoting the left lateral decubitus sleeping position have the potential to reduce nocturnal reflux symptoms. In a study, patients with nocturnal heartburn or regurgitation at least twice a week were instructed to sleep with a positional therapy device for 2 weeks. This device consisted of a wedge that created a 15-20° angle for the entire torso and a cushion to promote the left lateral decubitus position (Fig. 1). After 2 weeks of use, nocturnal reflux symptoms were significantly reduced and health-related quality of life increased. In another study with the same positional therapy device, it was concluded that it was also effective in reducing symptoms in 27 patients with laryngopharyngeal reflux39.
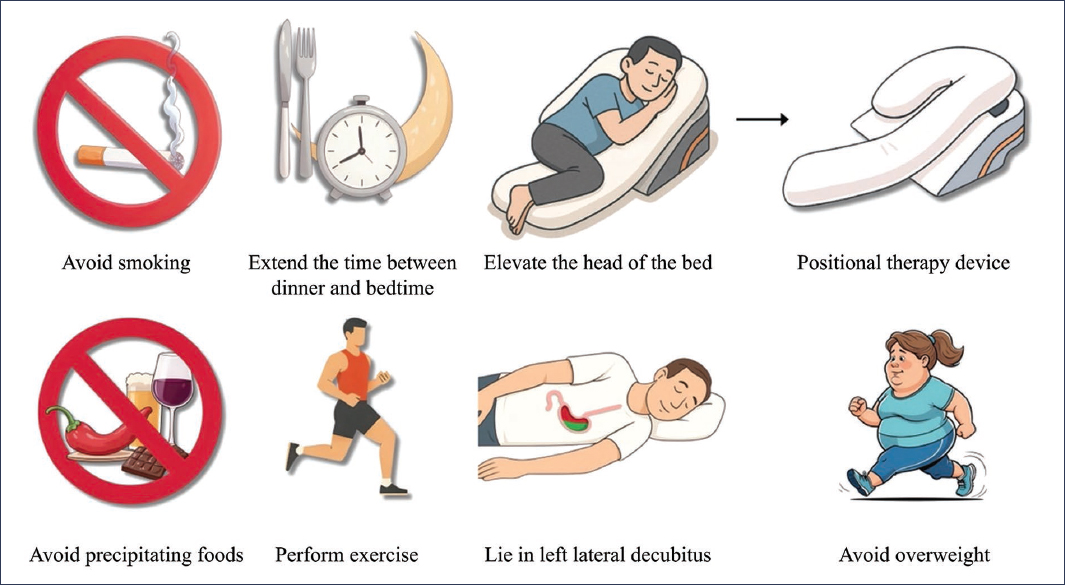
Figure 1. Lifestyle modifications in GERD.
Conclusions
Recent studies have established the importance of nutrition for managing GERD symptoms. There is increasing scientific evidence that has generated objective data on the role of certain trigger foods, while population studies support the reduction of reflux symptoms by following certain diets. Avoiding foods that can precipitate reflux symptoms can improve the patient’s quality of life. Obesity has also been linked to increased GERD symptoms; weight loss reduces esophageal acid exposure and reflux symptoms, even in non-obese GERD patients. Patients with GERD symptoms should be recommended measures such as avoiding eating dinner close to bedtime, elevating the head of the bed at least 20 cm, and sleeping in the left lateral decubitus position.
Funding
The author declares having received no funding for this study.
Conflicts of interest
The author declares having no conflicts of interest.
Ethical considerations
Protection of people and animals. The author declares that no experiments on human beings or animals have been conducted for this research.
Confidentiality, informed consent, and ethical approval. The study does not involve personal patient data or require ethical approval. SAGER guidelines do not apply.
Declaration on the use of artificial intelligence. The author declares that no type of generative artificial intelligence was used for the writing of this manuscript.
